
Cardiovascular Anatomy — MCQs

10 questions
Read Study NotesQ1
Posterior cardinal veins develop into:
Q2
All the following openings in the right atrium are guarded by a valve except
Q3
Left anterior descending artery is a direct branch of
Q4
What is the cardiothoracic ratio in children?
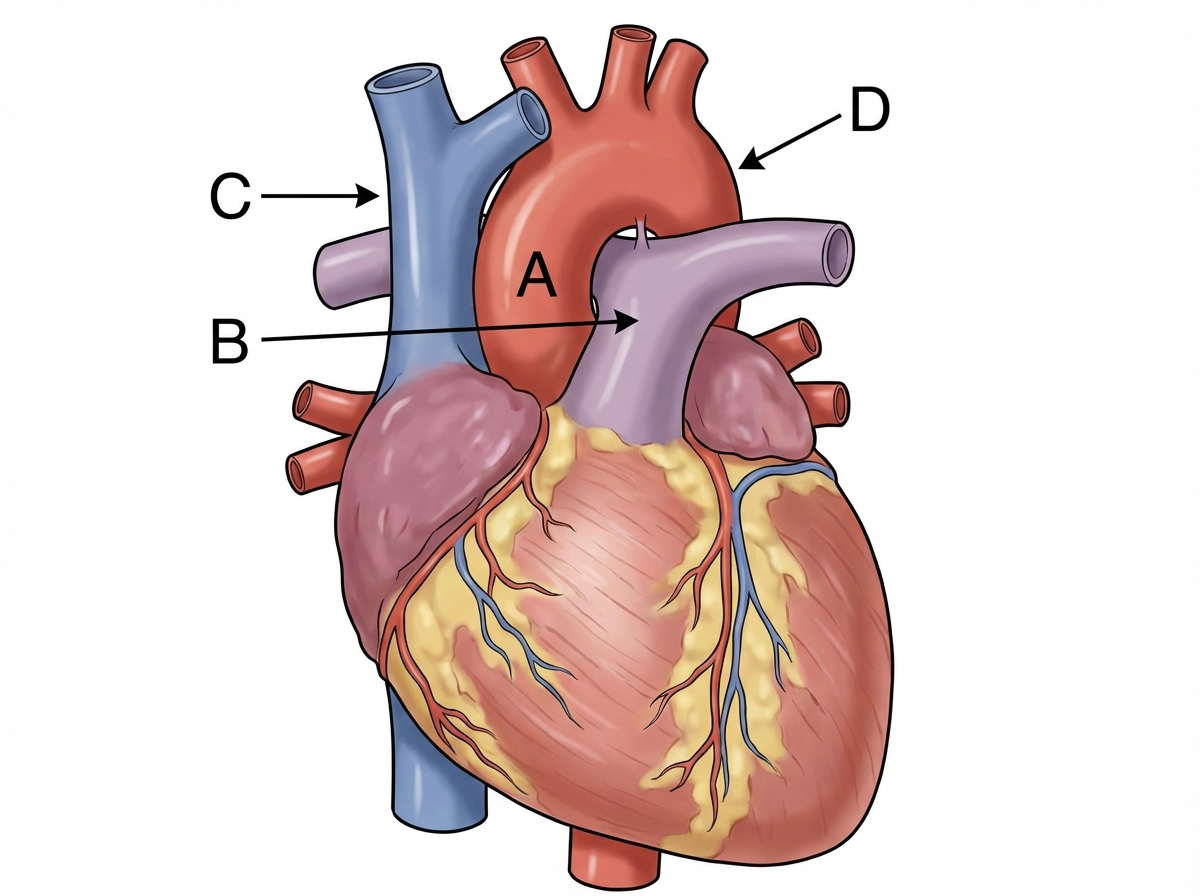
Q5
Identify the labeling correctly 
Q6
For pericardial calcifications, which is the best investigation?
Q7
Which X-ray finding is more characteristic of ASD compared to VSD?
Q8
All of the following arteries are common sites of occlusion by a thrombus except:
Q9
Which heart chamber has the thickest wall?
Q10
Keyhole sign on fetal ultrasound is seen in:

Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app