
Aortic and Great Vessel Imaging — MCQs

A patient presents with engorged neck veins, a blood pressure of 80/50 mmHg, and a pulse rate of 100 beats per minute following blunt trauma to the chest. The diagnosis is:
The procedure of choice for the evaluation of aortic aneurysms is -
A 68-year-old asymptomatic male is found to have an abdominal aortic aneurysm (AAA) measuring 4.5 cm on routine ultrasound screening. What is the most appropriate management?
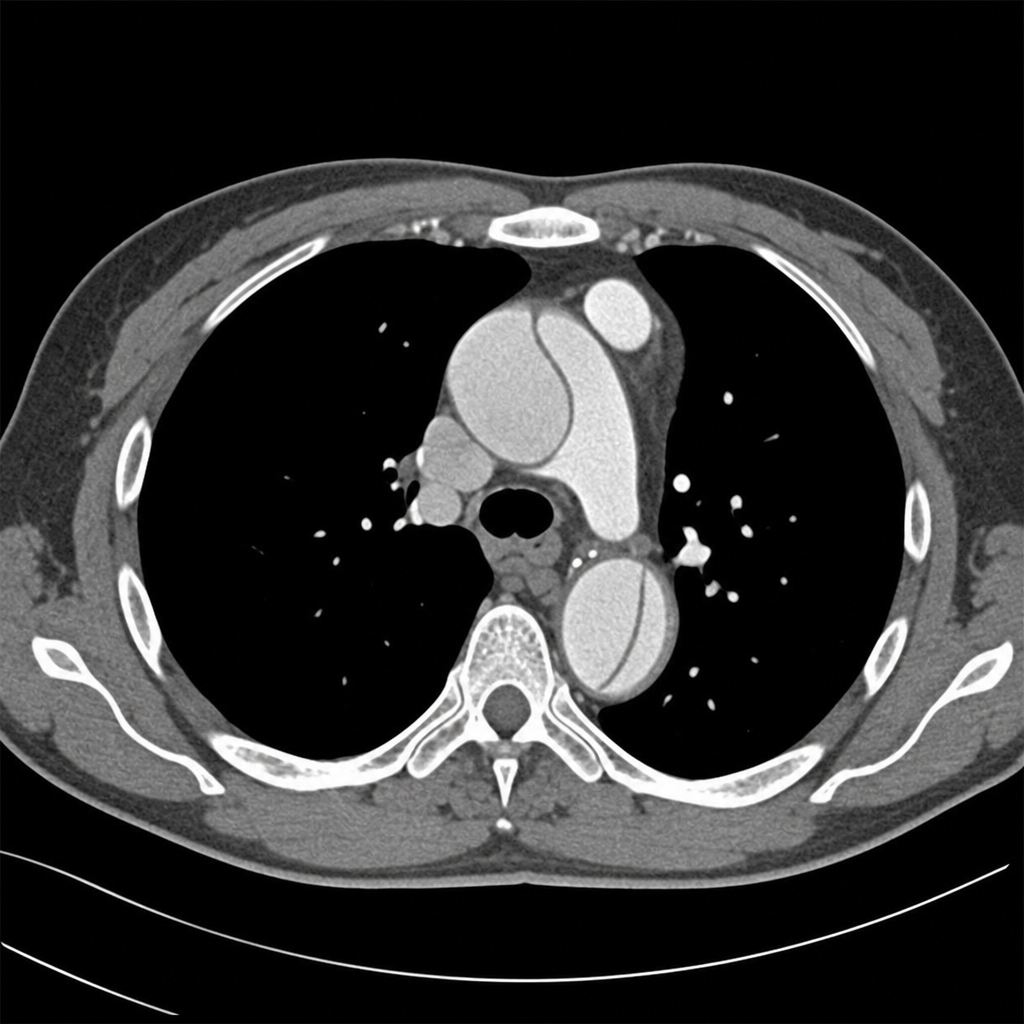
Comment on the diagnosis of the CT chest image shown below.
What is the cutoff for surgery in an abdominal aortic aneurysm in asymptomatic patients?
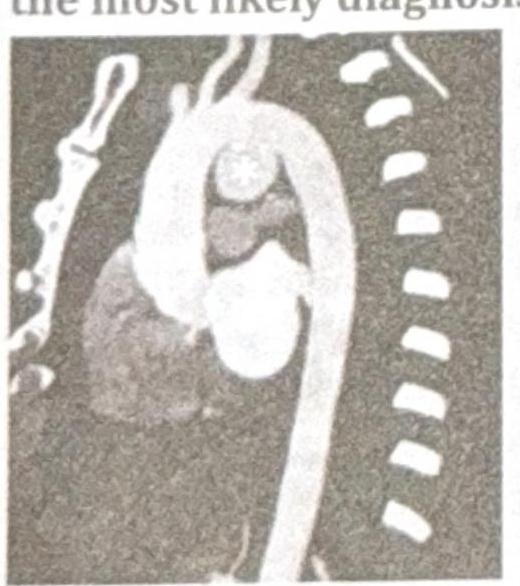
A 38-year-old patient presents with chest pain and hoarseness of voice for the past month. Based on the radiographic image below, what is the most likely diagnosis?
In Marfan's syndrome, Aortic aneurysm occurs most commonly in:
Single heart sound (S2) is heard in:
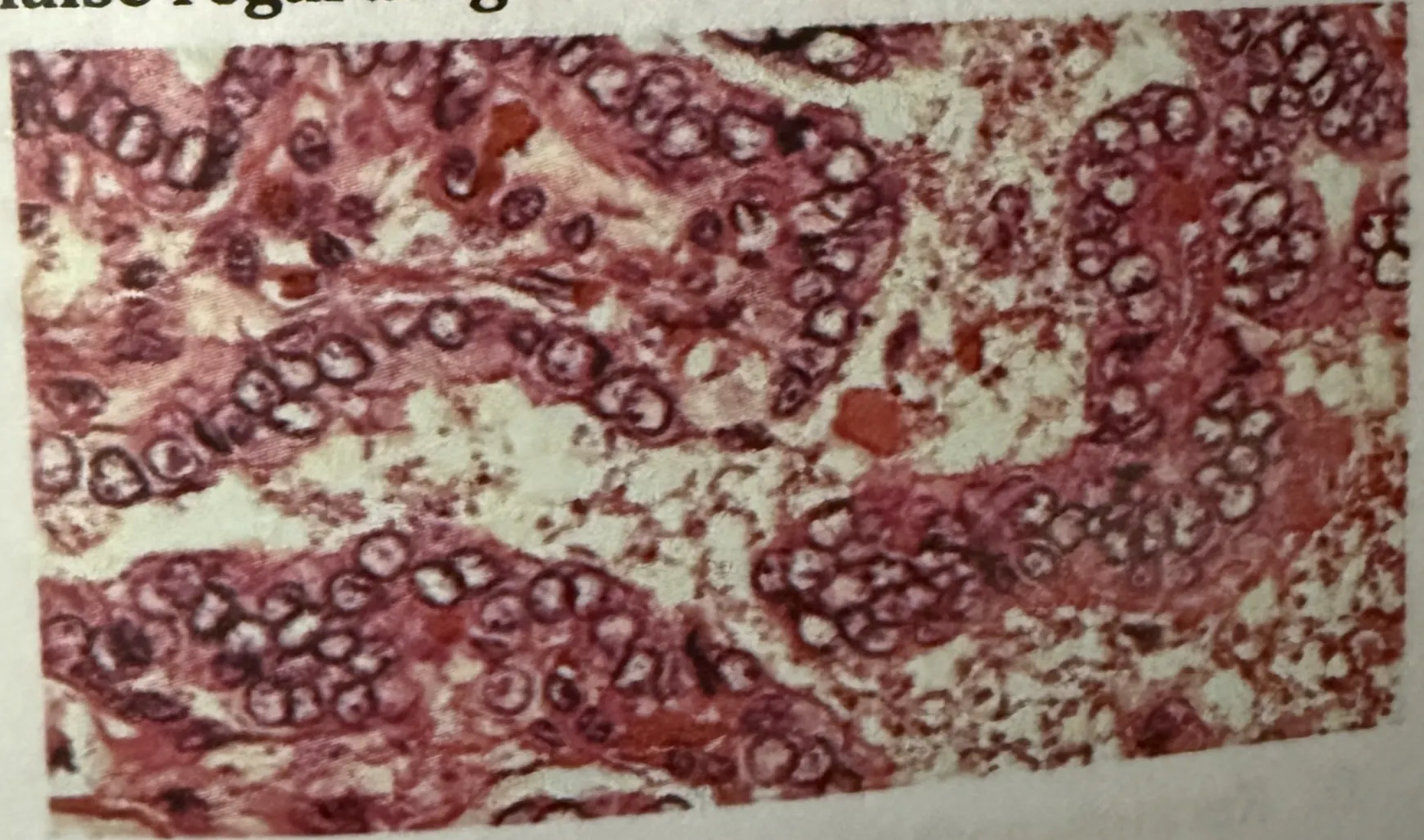
A middle aged male patient presents with painless slow growing neck swelling. On examination, lymph nodes are positive. Surgery is done and biopsy is shown in the image below. Which of the following is false regarding the HPE findings?
The thymus is located in which part of the body?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app