
Cardiovascular Radiology — MCQs

On this page
A young female undergoes renal angiography for evaluation of secondary hypertension. Based on her angiogram, what is the most likely diagnosis?
Which one of the following is used in Cardiovascular imaging?
Which of the following is NOT a characteristic feature of mitral stenosis on X-ray?
Which of the following statements is true regarding cardiac MRI?
A patient presents with chest pain. CT angiography demonstrates dilatation of the ascending aorta measuring 5.2 cm in diameter. What is the diagnosis?
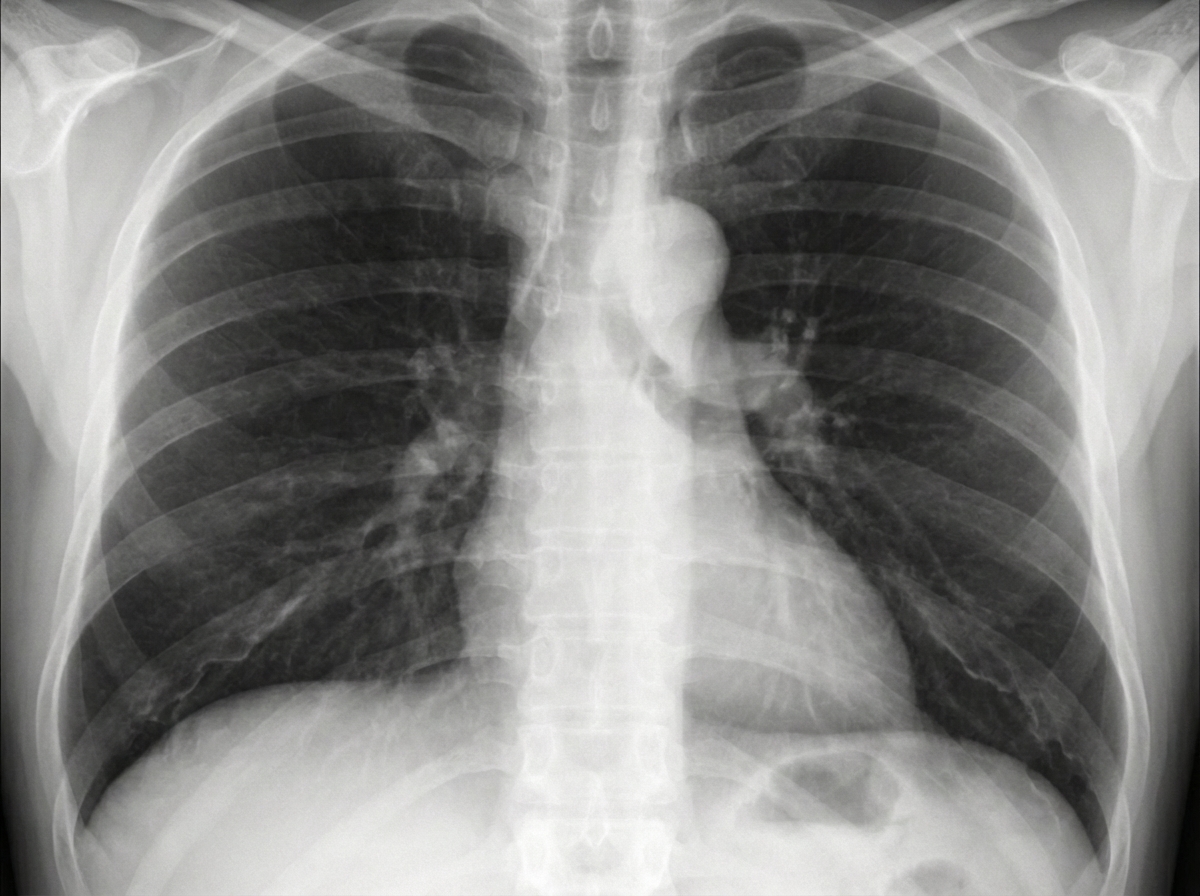
Which condition is associated with a 'figure of 8' appearance on a chest X-ray?
Classification of aortic dissection depends upon?
Which of the following is NOT a sign of right atrial enlargement?
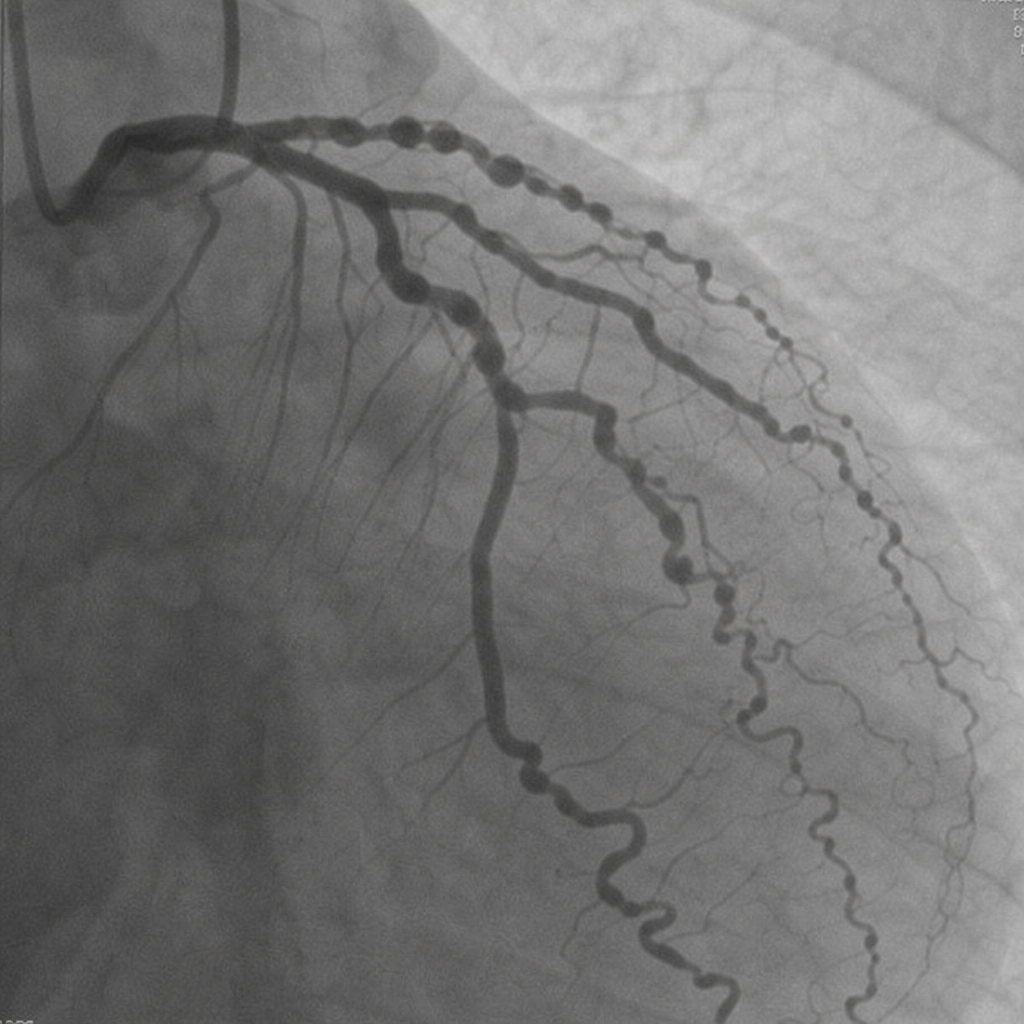
A 45-year-old man presents with hypertension, peripheral neuropathy, livedo reticularis, and elevated inflammatory markers. Urinalysis shows no red cell casts and no proteinuria. Renal angiography reveals multiple microaneurysms in the renal arteries. What diagnosis is suggested by the results of this coronary angiogram?
A triangular shaped heart is a radiological finding of which of the following conditions?
Practice by Chapter
Cardiovascular Anatomy
Practice Questions
Cardiac CT Techniques
Practice Questions
Cardiac MRI Techniques
Practice Questions
Ischemic Heart Disease Imaging
Practice Questions
Valvular Heart Disease
Practice Questions
Cardiomyopathies
Practice Questions
Pericardial Diseases
Practice Questions
Congenital Heart Disease
Practice Questions
Aortic and Great Vessel Imaging
Practice Questions
Peripheral Vascular Imaging
Practice Questions
Cardiovascular Interventional Procedures
Practice Questions
Post-Surgical Cardiovascular Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app