
Breast Imaging — MCQs

On this page
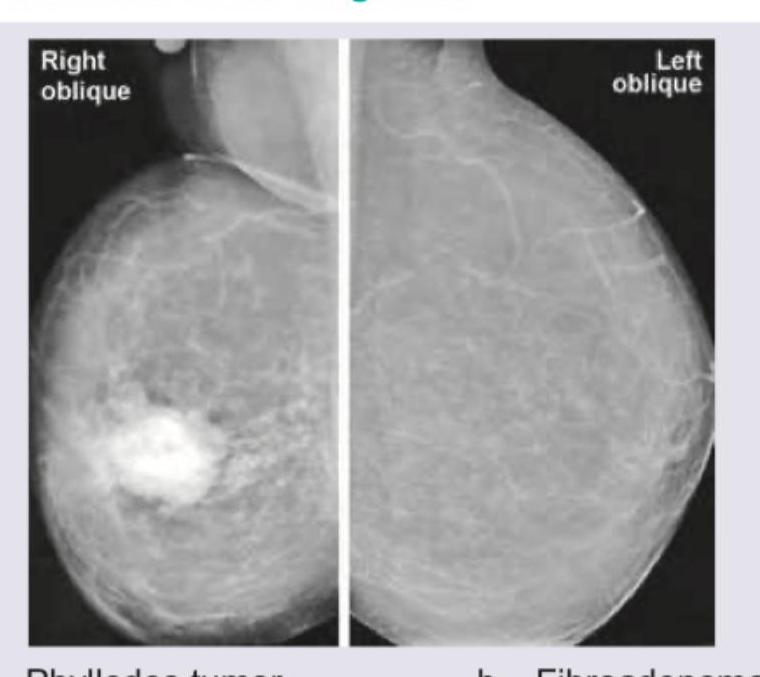
A 35-year-old woman presents with a rapidly enlarging palpable breast mass over the past 3 months. Mammography is performed. What is the most likely diagnosis?
Breast imaging reporting and data system (BI-RADS): Final assessment categorized a 45 year old female to have Category 5 disease. What does the report signify?
What is not an advantage of USG over mammography?
BIRADS stands for
Which of the following features on mammogram would suggest malignancy?
Which of the following features suggests a malignant lesion on mammography?
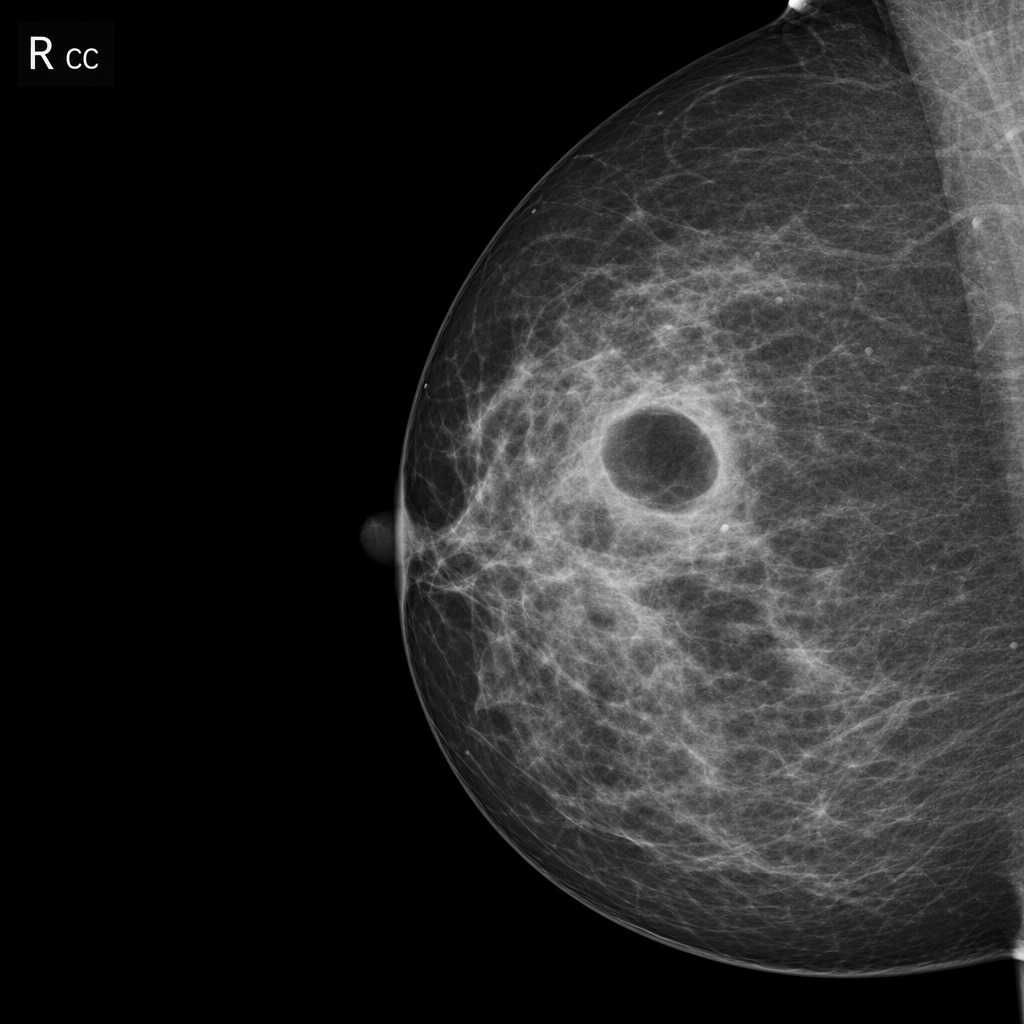
You are shown the screening mammogram of a 55-year-old woman. Which one of the following is the MOST likely diagnosis?
Fat-containing breast lesions are seen in:
Current gold standard to detect ductal carcinoma in situ breast is:
All of the following are true about mammography except -
Practice by Chapter
Breast Anatomy and Physiology
Practice Questions
Male Breast Imaging
Practice Questions
Mammography Techniques
Practice Questions
BI-RADS Classification
Practice Questions
Breast Ultrasonography
Practice Questions
Breast MRI
Practice Questions
Digital Breast Tomosynthesis
Practice Questions
Benign Breast Diseases
Practice Questions
Breast Cancer Detection and Diagnosis
Practice Questions
Interventional Breast Procedures
Practice Questions
Breast Cancer Screening
Practice Questions
Male Breast Imaging
Practice Questions
Post-treatment Breast Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app