
Breast Imaging — MCQs

On this page
"Linguine sign" and "Stepladder sign" that are specific for intracapsular breast implant rupture are both seen in:
Which of the following investigations is NOT indicated in a lactating woman presenting with painful breasts?
What does BI-RADS 4 classification indicate for a breast lesion?
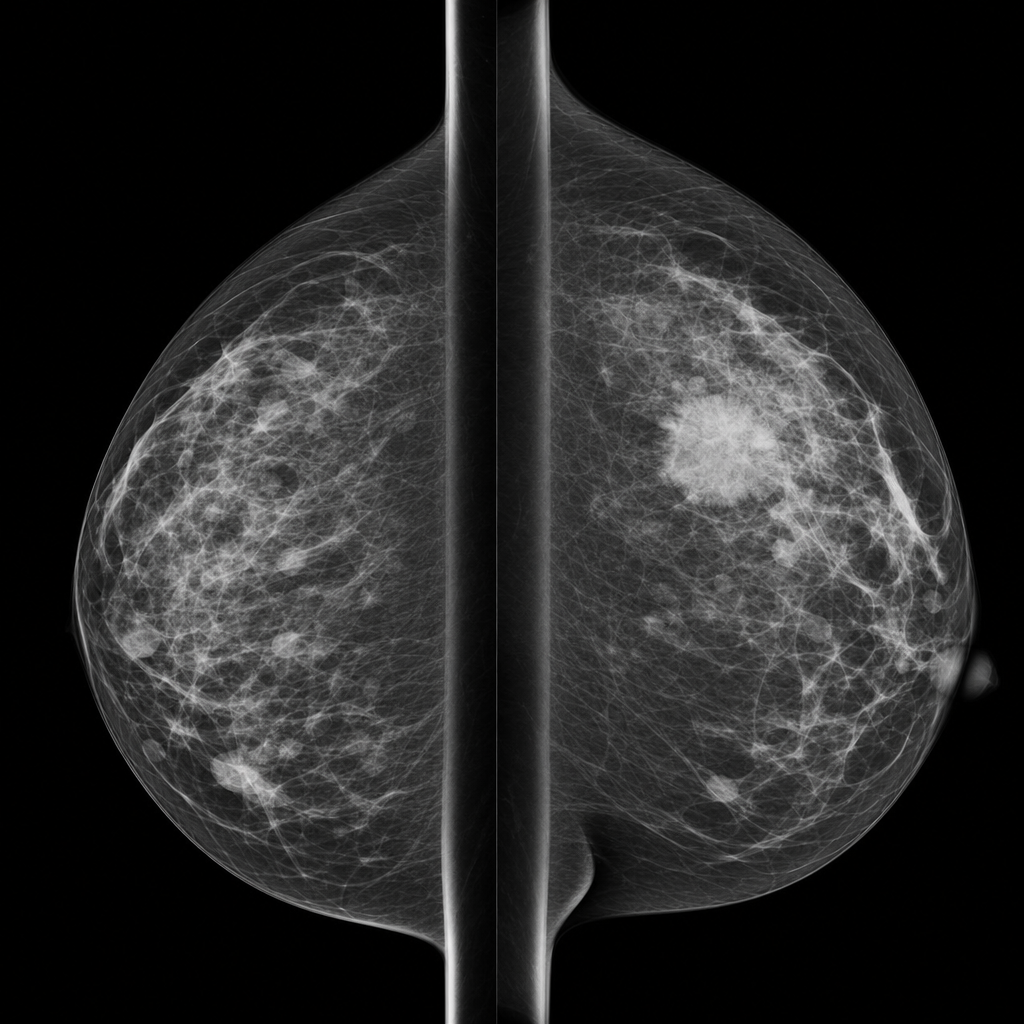
A 55-year-old post-menopausal woman, on hormone replacement therapy, presents with heaviness in both breasts. A screening mammogram reveals a high density speculated mass with a cluster of pleomorphic microcalcification and ipsilateral large axillary lymph nodes. The mass described here most likely represents?
A 55-year-old post-menopausal woman, on hormone replacement therapy (HRT), presents with heaviness in both breasts. A screening mammogram reveals a high density speculated mass with a cluster of pleomorphic microcalcification and ipsilateral large axillary lymph nodes. The mass described here most likely represents?
What are the standard views for mammography?
What is the investigation performed?
What is true about screening mammography?
Diffuse increase in the parenchymal density of the breast is seen in which of the following conditions?
What is the investigation of choice for high-risk breast cancer in a female?
Practice by Chapter
Breast Anatomy and Physiology
Practice Questions
Male Breast Imaging
Practice Questions
Mammography Techniques
Practice Questions
BI-RADS Classification
Practice Questions
Breast Ultrasonography
Practice Questions
Breast MRI
Practice Questions
Digital Breast Tomosynthesis
Practice Questions
Benign Breast Diseases
Practice Questions
Breast Cancer Detection and Diagnosis
Practice Questions
Interventional Breast Procedures
Practice Questions
Breast Cancer Screening
Practice Questions
Male Breast Imaging
Practice Questions
Post-treatment Breast Imaging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app