
Biliary Tract Imaging — MCQs

Causes of thickened gallbladder wall on ultrasound examination are all except:
The X-ray appearance of a CBD stone on cholangiography is:
What is the best way to diagnose gallbladder stones?
Which of the following is not a risk factor for cholangiocarcinoma?
In a patient presenting with jaundice, the HIDA scan would be most useful for which of the following:
Which of the following statements about CT imaging is the MOST accurate?
What is the investigation of choice in a patient with blunt abdominal trauma with hematuria?
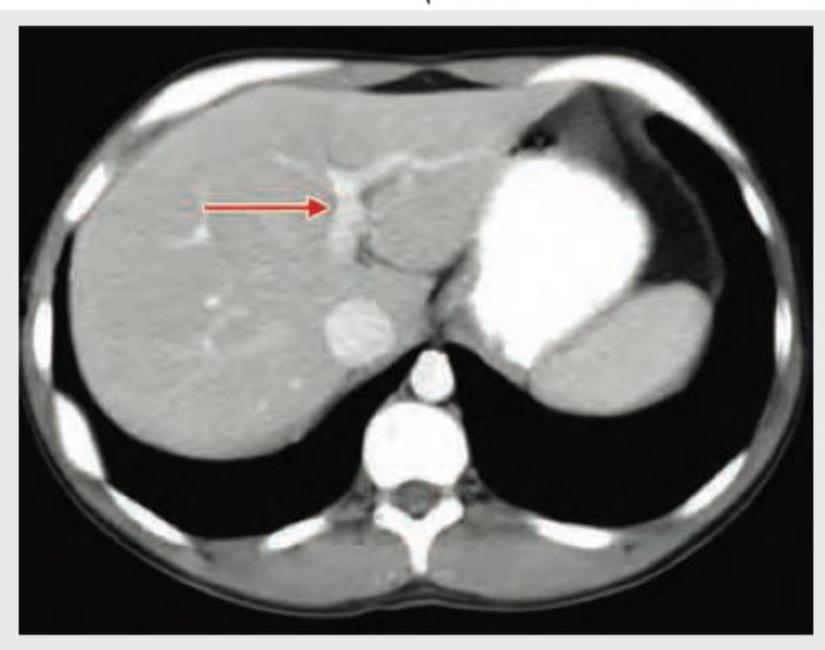
Identify the structure shown in CT abdomen section. (Recent NEET Pattern 2018-19)
Causes of thickened gallbladder wall on ultrasound examination are all except:
The following IVU shows:

Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app