
Adrenal Imaging — MCQs

A patient presents with headaches, palpitations, hypertension, and urine VMA positivity. The biopsy findings are shown in the image. Which of the following statements is correct?
Pheochromocytoma is characterized by excessive secretion of:
What is the Diagnosis based on the CT Scan given below?
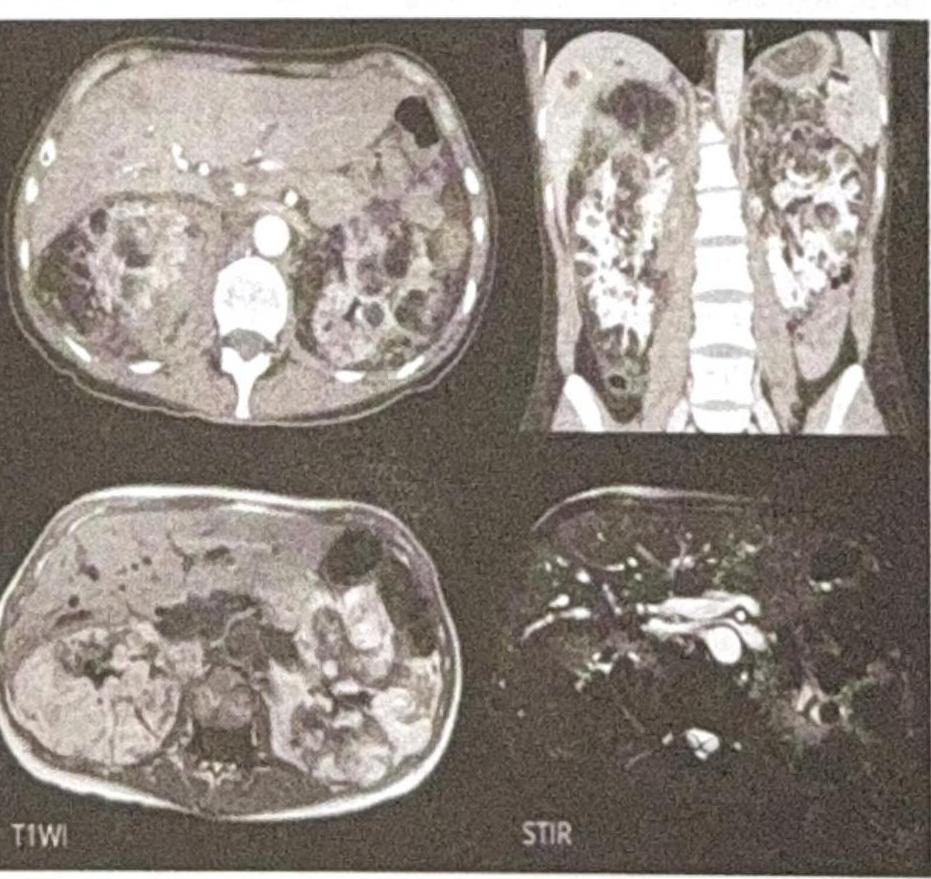
Enhancement in CT contrast is due to -
Which of the following statements about CT imaging is the MOST accurate?
What is the best investigation for diagnosis and staging of renal cell carcinoma with thrombus extending into the IVC?
A patient presents with right iliac fossa pain for 48 hours. USG image (shown with Doppler) demonstrates a hyperaemic appendix-region structure with surrounding inflammatory changes. There is no free fluid or evidence of perforation on USG. What is the most appropriate next step?
An elderly female patient presents to the emergency department with acute onset left flank pain radiating to the groin. What is the most appropriate imaging protocol for initial evaluation?
A 58-year-old male presents with a 3-month history of altered bowel habits, passage of blood mixed with stool, and a 6 kg weight loss. Colonoscopy was incomplete due to a tight stricture in the sigmoid colon. A barium enema is performed and the image is shown in Image 3. Which radiological sign is demonstrated, and with which pathology is it classically associated?

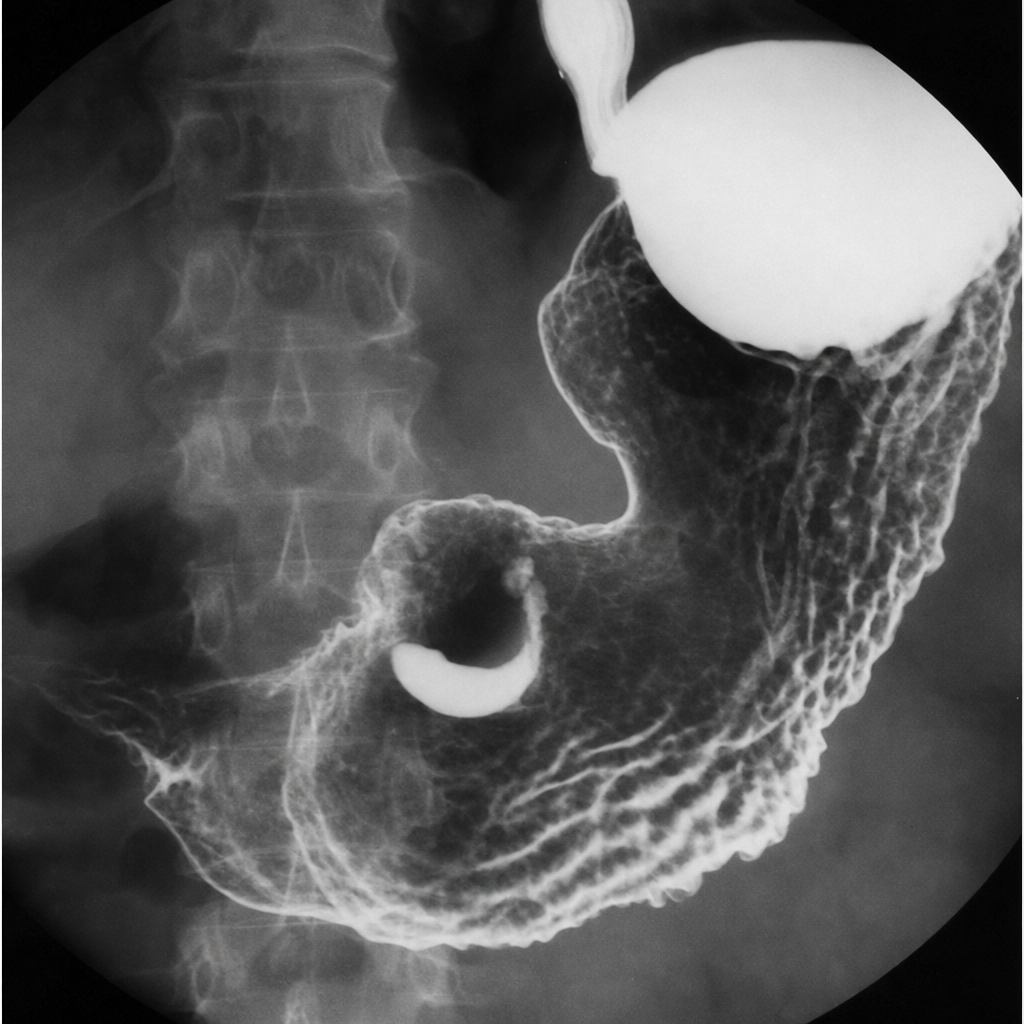
A 65-year-old male presents with a 4-month history of epigastric pain, early satiety, and progressive weight loss. He has a history of Helicobacter pylori infection treated 10 years ago. Haemoglobin is 9.2 g/dL. A barium meal fluoroscopy study is shown in Image 1. Which of the following best describes the radiological sign visible and its significance?
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app