
Substance Use Disorders — MCQs

On this page
Physical withdrawal symptoms are not marked in patients abusing which of the following substances?
Which of the following is a symptom of opioid withdrawal?
A 35-year-old man presented with agitation, global confusion, disorientation, hallucinations, and autonomic hyperactivity. He had his last alcohol drink 5 days ago. Which of the following can be used in the immediate treatment of the condition?
A patient consuming 120 ml of alcohol daily for the past 12 years is diagnosed with alcohol-dependent syndrome. Which of the following drugs should be avoided in its management?
All of the following are used for the treatment of morphine dependence except?
Which of the following is NOT a feature of caffeine withdrawal?
A 45-year-old alcoholic male presents for deaddiction treatment. He has alcohol-induced hepatitis with other blood parameters within normal limits. Which drug should NOT be chosen for relapse prevention?
A patient with a known history of alcohol dependence develops seizures for the first time 12 to 18 hours after their last drink. The LFTs are within normal limits. What is the most appropriate pharmacological treatment for this patient?
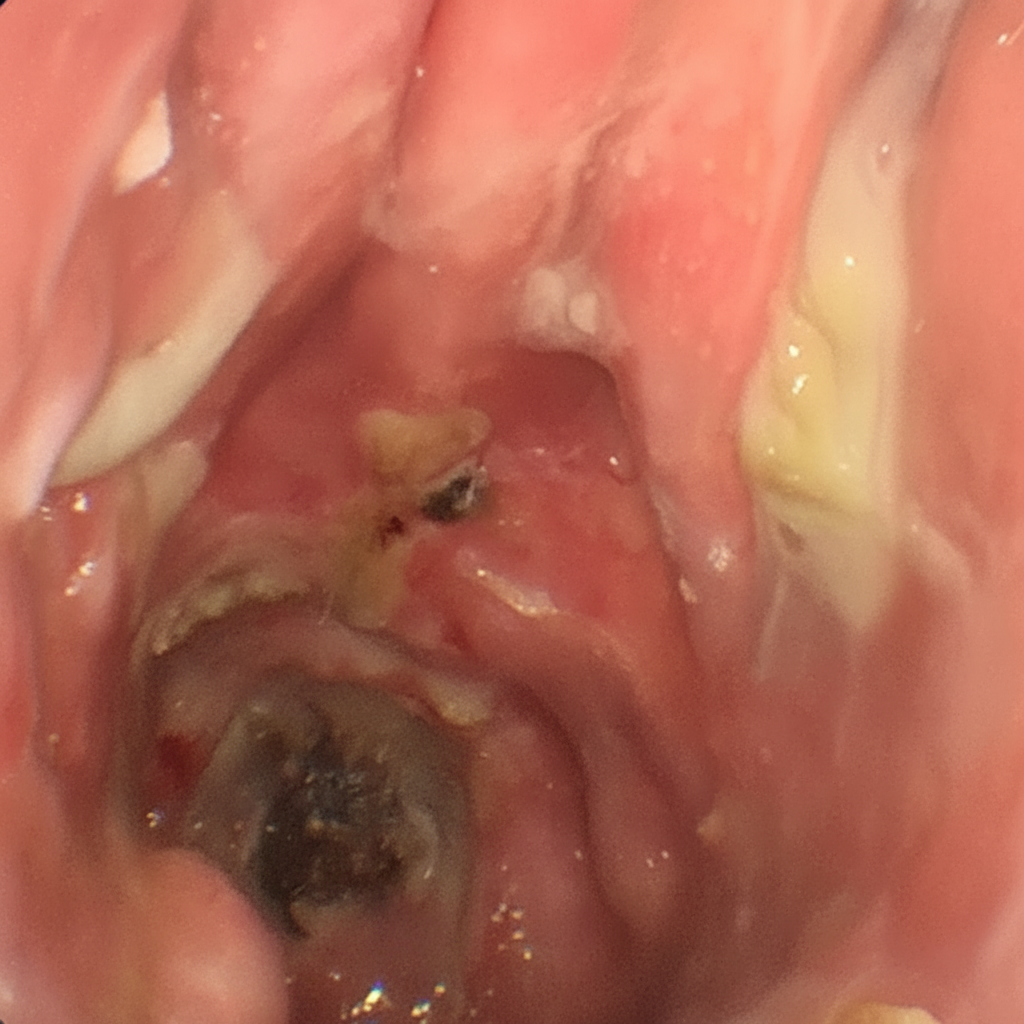
Which one of the following drugs of abuse is most typically associated with the illustrated complication?
Withdrawal of which of the following substances causes piloerection?
Practice by Chapter
Neurobiology of Addiction
Practice Questions
Alcohol Use Disorder
Practice Questions
Opioid Use Disorder
Practice Questions
Cannabis Use Disorder
Practice Questions
Stimulant Use Disorders
Practice Questions
Sedative, Hypnotic, and Anxiolytic Use Disorders
Practice Questions
Tobacco Use Disorder
Practice Questions
Hallucinogen-Related Disorders
Practice Questions
Substance Withdrawal Syndromes
Practice Questions
Pharmacotherapy for Substance Use Disorders
Practice Questions
Psychosocial Interventions
Practice Questions
Dual Diagnosis Management
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app