
Sleep-Related Movement Disorders — MCQs

All are true about management of PDPH except-
A 32-year-old patient with Restless leg syndrome comes to the OPD. What is the most appropriate first line treatment?
A 42-year-old female executive is referred to the sleep clinic with jaw pain. She complains that after she arrives home at night around 10 pm she frequently drinks 3-4 gin and tonics to help quiet her mind.’ She wakes up the next morning around 3am to read the international stock market news, at which point she states her teeth ache an unbearable amount. A study is performed on the patient and it is noted that she grinds her teeth and mutters during roughly half of her sleep. Which of the following would you expect to see on her EEG and at which stage of sleep would you expect her jaw pain to be caused?
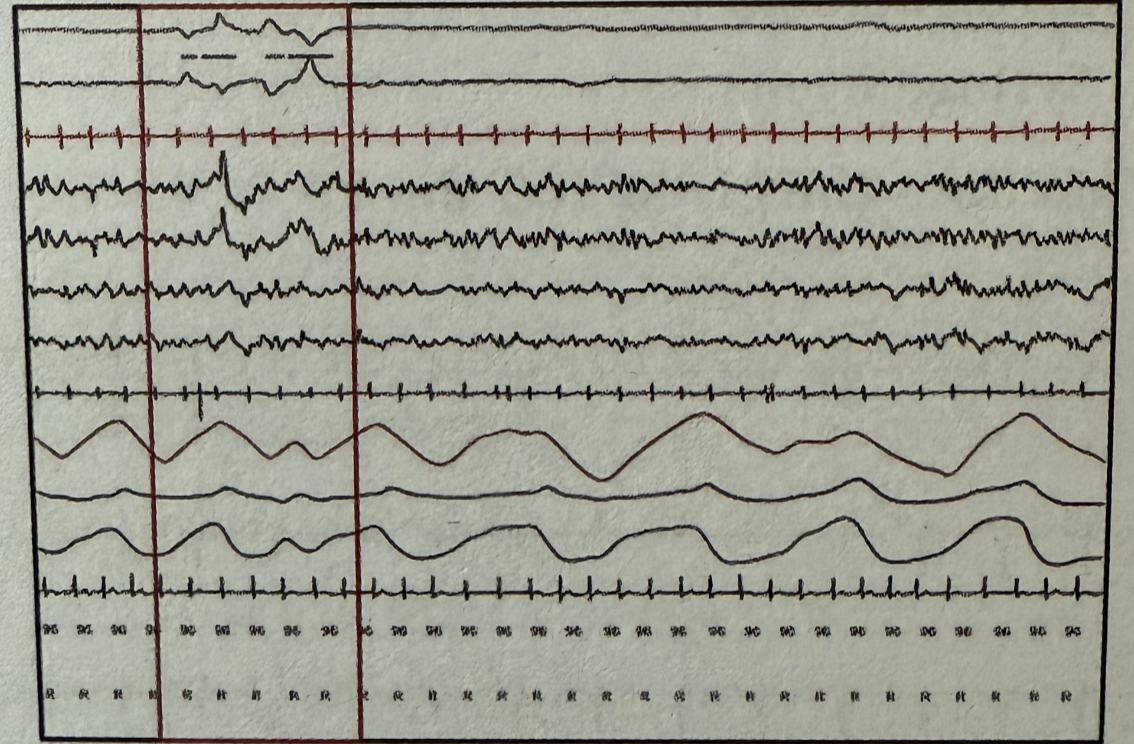
During polysomnography, which stage of sleep is represented by the marked areas when observing the following wave patterns? EOG (Electrooculography) EEG (Electroencephalography) EMG (Electromyography)
In narcolepsy, the polysomnographic recording typically shows which of the following patterns?
Somnambulism is mostly seen in which age group?
An otherwise healthy 43-year-old woman comes to the physician because of several episodes of involuntary movements of her head over the past few months. They are sometimes associated with neck pain and last minutes to hours. Neurologic examination shows no abnormalities. During examination of the neck, the patient's head turns horizontally to the left. She states this movement is involuntary, and that she is unable to unturn her head. After 5 minutes, her head re-straightens. Which of the following best describes this patient's disorder?
Chorea is NOT seen in
A patient was recently started on Fluphenazine. A few weeks later, he developed tremors, rigidity, bradykinesia, and excessive salivation. The first line of management for this patient is
The term 'cocaine bugs' refers to:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app