
Psychopharmacology — MCQs

On this page
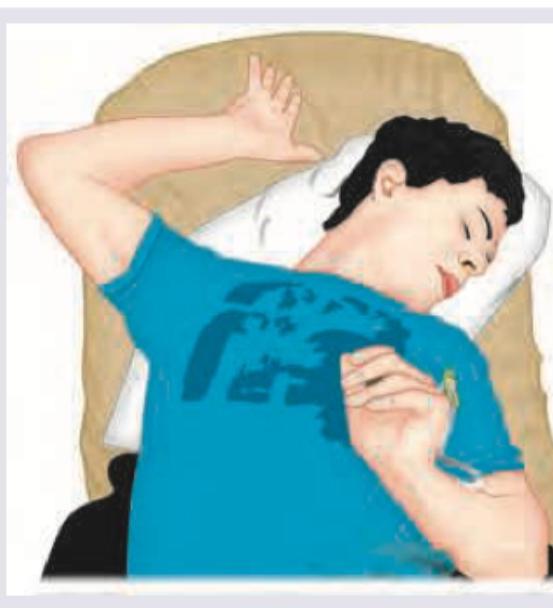
A 25-year-old uncooperative patient of schizophrenia was brought in to the casualty. The Casualty Medical Officer gave an injectable drug to the patient. Two hours later patient develops the following posturing. What is the best treatment among the options listed?
Which of the following medications may be used in a child diagnosed with Attention Deficit Hyperactivity Disorder? I. Carbamazepine II. Methylphenidate III. Atomoxetine IV. Clonazepam Select the correct answer using the code given below :
A 29 year old lady came to psychiatry OPD with symptoms of hypomania. She has a past history of manic episode. Now, she is planning to conceive. Which drug should be avoided for being highly teratogenic to the fetus?
A patient of schizophrenia is being treated with clozapine. For which rare but serious side effects should he be monitored?
Which of the following is not an off-label use of risperidone?
A 22-year-old woman presents with a complaint of low energy levels for the past 6 months. She feels as if she has no energy to do anything and has lost interest in photography, which she was previously passionate about. Feelings of hopelessness occupy her mind and she can no longer focus at work. She says she forces herself to hang out with her friends at weekends but would rather stay home. She denies any suicidal ideation. Her past medical history is significant for bulimia nervosa, which was diagnosed when she was a teen and was controlled with cognitive behavioral therapy. In addition, she has gastroesophageal reflux, which is being treated with esomeprazole. The patient has a 10-pack-year smoking history but denies any alcohol or recreational drug use. On examination, she is afebrile and vital signs are within normal limits. Her BMI is 24 kg/m2. Further physical examination is unremarkable. Which of the following aspects of this patient’s history is a contraindication to using bupropion as an antidepressant?
Drug of choice for treatment of akathisia is:-
All are used in attention deficit hyperactivity disorder (ADHD) except:
Drug of choice for obsessive-compulsive disorder
Drugs used in ADHD are:
Practice by Chapter
Principles of Psychopharmacology
Practice Questions
Antipsychotic Medications
Practice Questions
Antidepressant Medications
Practice Questions
Mood Stabilizers
Practice Questions
Anxiolytics and Hypnotics
Practice Questions
Stimulants and Cognitive Enhancers
Practice Questions
Pharmacokinetics and Pharmacodynamics
Practice Questions
Drug Interactions
Practice Questions
Adverse Effects and Management
Practice Questions
Pharmacogenomics in Psychiatry
Practice Questions
Special Populations Considerations
Practice Questions
Treatment Algorithms and Guidelines
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app