
Psychopharmacology — MCQs

On this page
Lithium is used in the prophylactic treatment of which of the following conditions?
Which of the following are pharmacologically approved treatments for tobacco addiction?
What is the therapeutic serum level of lithium in acute mania?
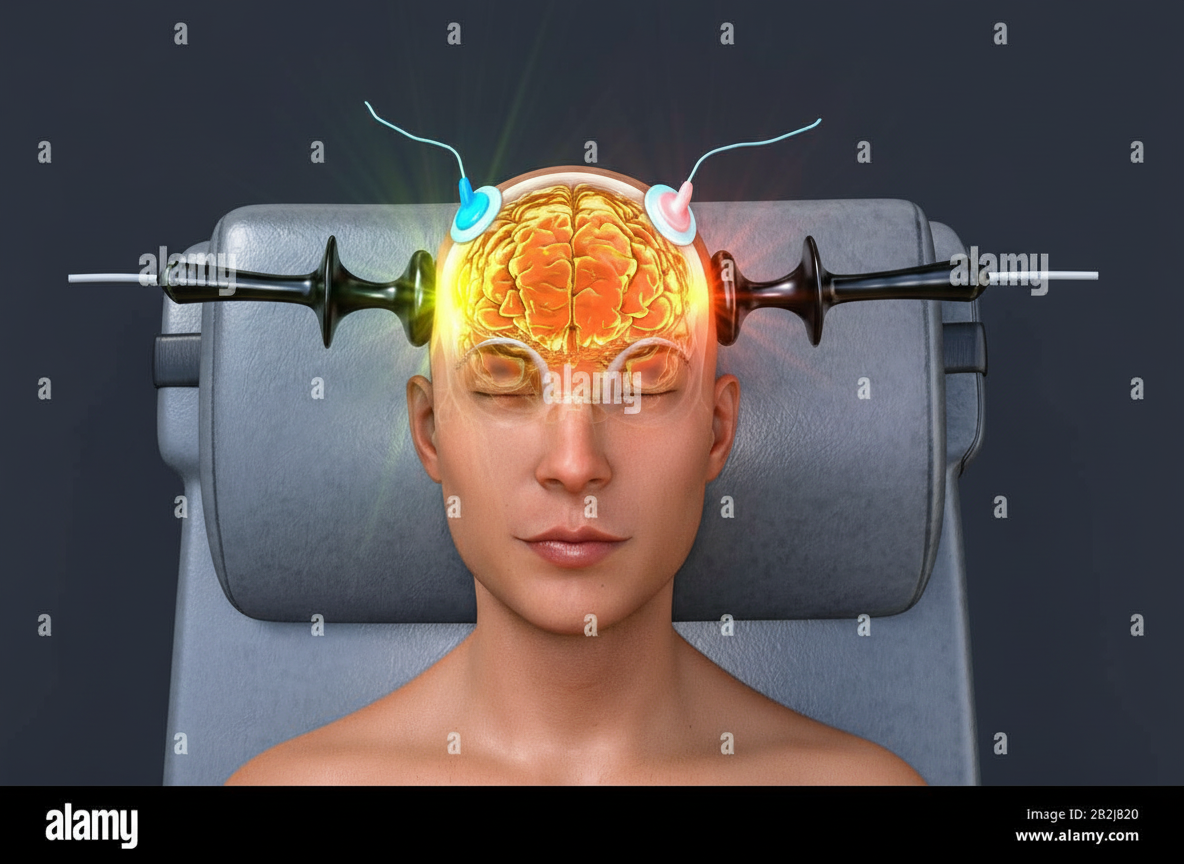
The procedure shown below is used in all of the following illnesses except:
A 28-year-old woman with bipolar disorder has a lithium level of 2.3 mEq/L (normal range 0.6-1.25 mEq/L). Which of the following side effects is most likely to occur?
Raj Mohan has recently been on an increased regime of antipsychotics for Schizophrenia. Which of the following complications is NOT associated with the combined use of more than one antipsychotic?
A 60-year-old male presents with profound guilt, believing he has committed sins throughout his life. He exhibits depressive symptoms and has contemplated suicide. He has sought guidance from a spiritual guru and is resistant to reassurance from his wife about his virtuous life. How would you manage this patient?
Who introduced lithium for the treatment of manic-depressive illness?
Which of the following drugs are used for recurrent depressive episodes?
Which of the following conditions increases the chance of hyponatremia in a patient treated with an antidepressant?
Practice by Chapter
Principles of Psychopharmacology
Practice Questions
Antipsychotic Medications
Practice Questions
Antidepressant Medications
Practice Questions
Mood Stabilizers
Practice Questions
Anxiolytics and Hypnotics
Practice Questions
Stimulants and Cognitive Enhancers
Practice Questions
Pharmacokinetics and Pharmacodynamics
Practice Questions
Drug Interactions
Practice Questions
Adverse Effects and Management
Practice Questions
Pharmacogenomics in Psychiatry
Practice Questions
Special Populations Considerations
Practice Questions
Treatment Algorithms and Guidelines
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app