
Psychiatric Assessment and Diagnosis — MCQs

On this page
A doctor asked the patient what her age is and she told him that she is married to an older man, and she has 2 kids of 15 and 18 years, and she is 39 years old. What is the disorder present?
Which of the following does not suggest a medical cause of mental illness?
The Mental State Examination (100-7) examines which of the following mental functions?
A patient with schizophrenia says, "Lord Hanuman was celibate, I am celibate too, so I am Lord Hanuman." Which thought abnormality is present in this patient?
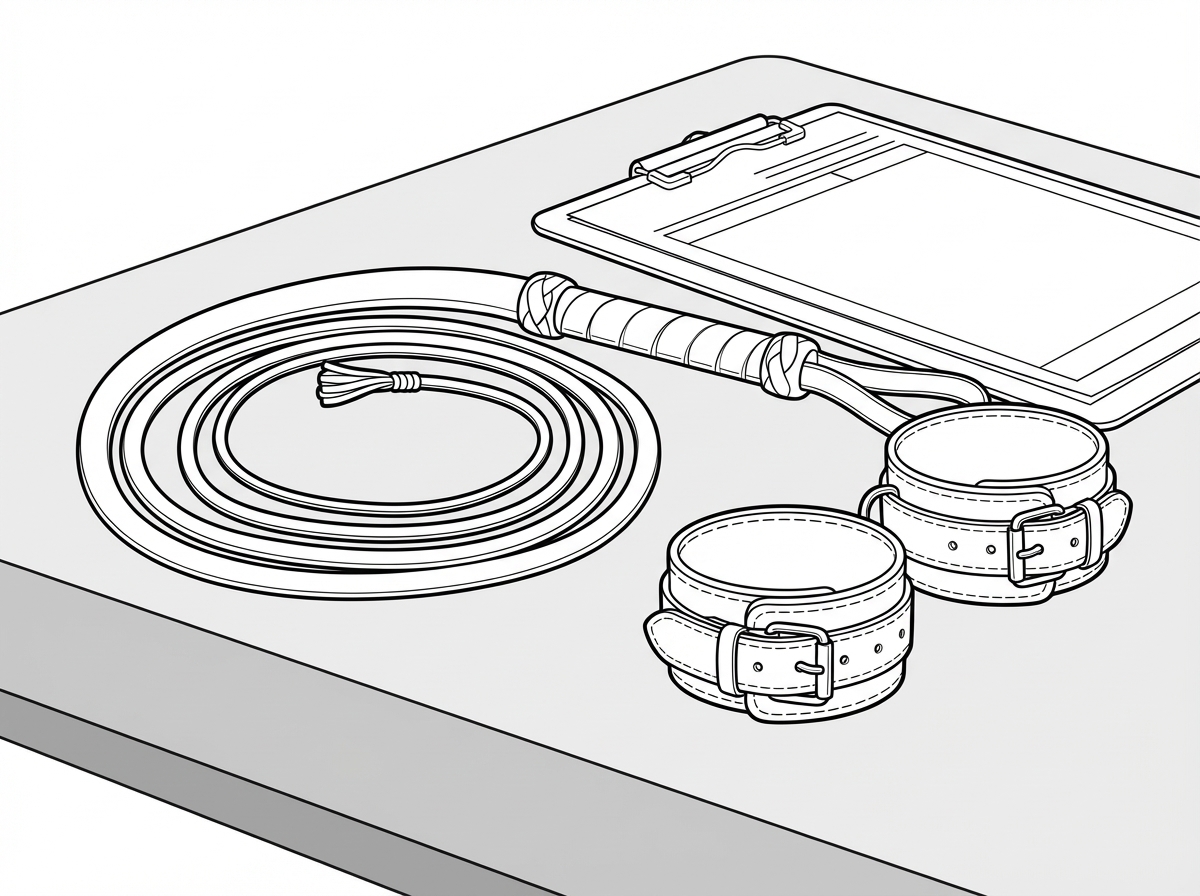
What is the sexual perversion depicted below?
The 4AT is a screening tool for detection of delirium. Which THREE of the following parameters listed below are included in the 4AT tool? I. Alertness II. Apnoea III. Abbreviated Mental Test (AMT4) IV. Attention Select the correct answer using the code given below:
Which of the following are clinical features of Fronto-Temporal dementia ? I. Personality change II. Language disturbance III. Memory may be preserved in early stages IV. Anti-cholinesterases are the drug of choice for treatment Select the correct answer using the code given below :
A patient with schizophrenia is asked to participate in a minimal-risk observational study. The patient demonstrates good understanding of the study procedures and potential benefits but has some difficulty with abstract concepts. Analyze the capacity determination for research participation.
A 75-year-old patient with mild cognitive impairment is asked to participate in a clinical trial. The patient shows variable understanding of the study when questioned at different times. Family members are eager for the patient to participate. Analyze the ethical considerations in determining study eligibility.
A 17-year-old patient presents with depression and suicidal ideation. The patient's parents want to be informed about all treatment decisions, but the patient refuses to allow disclosure. The patient demonstrates good understanding of treatment options. Analyze the competing ethical principles and determine the most appropriate course of action.
Practice by Chapter
Clinical Interview Techniques
Practice Questions
Mental Status Examination
Practice Questions
Diagnostic Formulation
Practice Questions
Rating Scales and Questionnaires
Practice Questions
Psychological Testing
Practice Questions
Neuropsychological Assessment
Practice Questions
Risk Assessment
Practice Questions
Laboratory Investigations in Psychiatry
Practice Questions
Neuroimaging in Clinical Assessment
Practice Questions
Cultural Considerations in Assessment
Practice Questions
Developmental Assessment
Practice Questions
Diagnostic Classification Systems
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app