
Psychiatric Assessment and Diagnosis — MCQs

On this page
Which of the following is NOT a feature of hallucination?
Which one of the following disorders is related to a sense of unreality?
Hallucinations are defined as:
What is hypomimia?
Which bedside test is primarily used to assess mental status?
A patient was asked a direct question about her age. Instead, she provided excessive and unnecessary details about her marriage and children before eventually answering the question. This is characteristic of which speech pattern?
A doctor asked the patient what her age is and she told him that she is married to an older man, and she has 2 kids of 15 and 18 years, and she is 39 years old. What is the disorder present?
Which of the following does not suggest a medical cause of mental illness?
The Mental State Examination (100-7) examines which of the following mental functions?
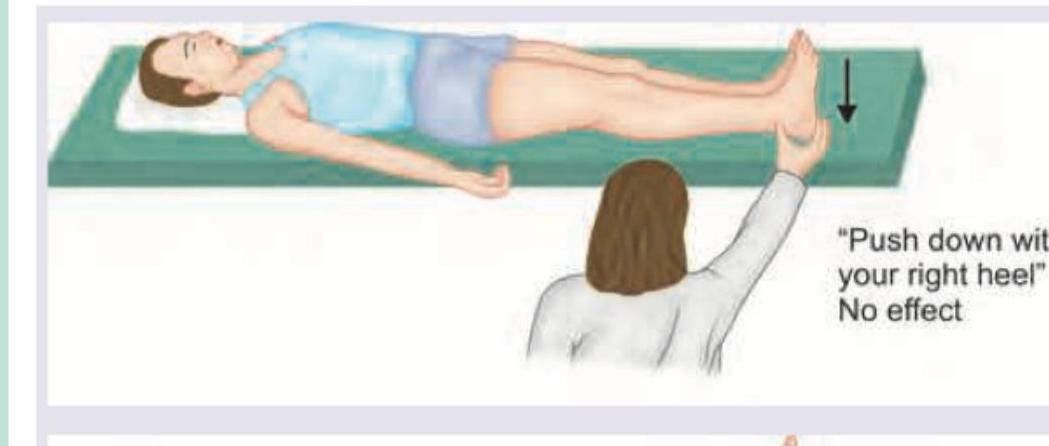
Comment on the test being performed in the patient.
Practice by Chapter
Clinical Interview Techniques
Practice Questions
Mental Status Examination
Practice Questions
Diagnostic Formulation
Practice Questions
Rating Scales and Questionnaires
Practice Questions
Psychological Testing
Practice Questions
Neuropsychological Assessment
Practice Questions
Risk Assessment
Practice Questions
Laboratory Investigations in Psychiatry
Practice Questions
Neuroimaging in Clinical Assessment
Practice Questions
Cultural Considerations in Assessment
Practice Questions
Developmental Assessment
Practice Questions
Diagnostic Classification Systems
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app