
Thermoregulation — MCQs

On this page
Which of the following is endogenous pyrogen?
Fever increases water loss by how much for each degree Celsius increase in body temperature?
What is the primary mechanism underlying hyperthermia?
During acclimatization to hot environments, increased sweating efficiency is primarily due to enhanced sensitivity of which receptors?
Lesion of preoptic nucleus of hypothalamus is associated with which of the following conditions?
Nonshivering thermogenesis in adults is due to:
Shivering is controlled by?
The temperature centre is?
What is the PRIMARY pathophysiological feature that defines severe heat stress?
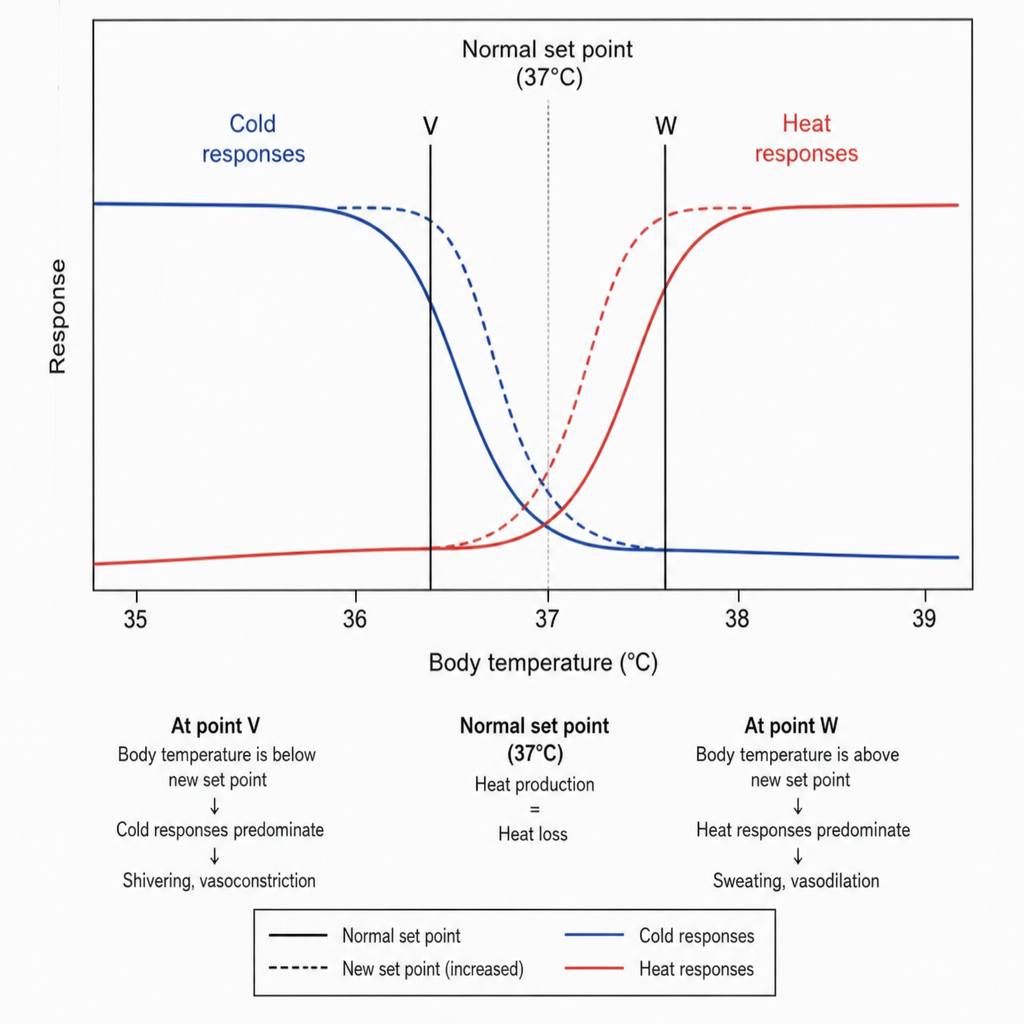
The diagram shows the effects of changing the set point of the hypothalamic temperature controller. Which set of changes occurs at point W compared with point V?
Practice by Chapter
Heat Production and Loss
Practice Questions
Temperature Sensing Mechanisms
Practice Questions
Hypothalamic Regulation of Temperature
Practice Questions
Behavioral Thermoregulation
Practice Questions
Fever and Hyperthermia
Practice Questions
Hypothermia
Practice Questions
Exercise and Thermoregulation
Practice Questions
Thermoregulation in Extreme Environments
Practice Questions
Age-Related Changes in Thermoregulation
Practice Questions
Disorders of Thermoregulation
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app