
Sensory Systems — MCQs

On this page
A lesion in the posterior column of the spinal cord will affect which of the following modalities?
Tapping the patellar tendon with a reflex hammer produces a brief contraction of the knee extensors. What is the cause of this muscle contraction?
Pain is appreciated when the small bowel is
All are required for balancing EXCEPT:
Which of the following statements regarding color vision is true?
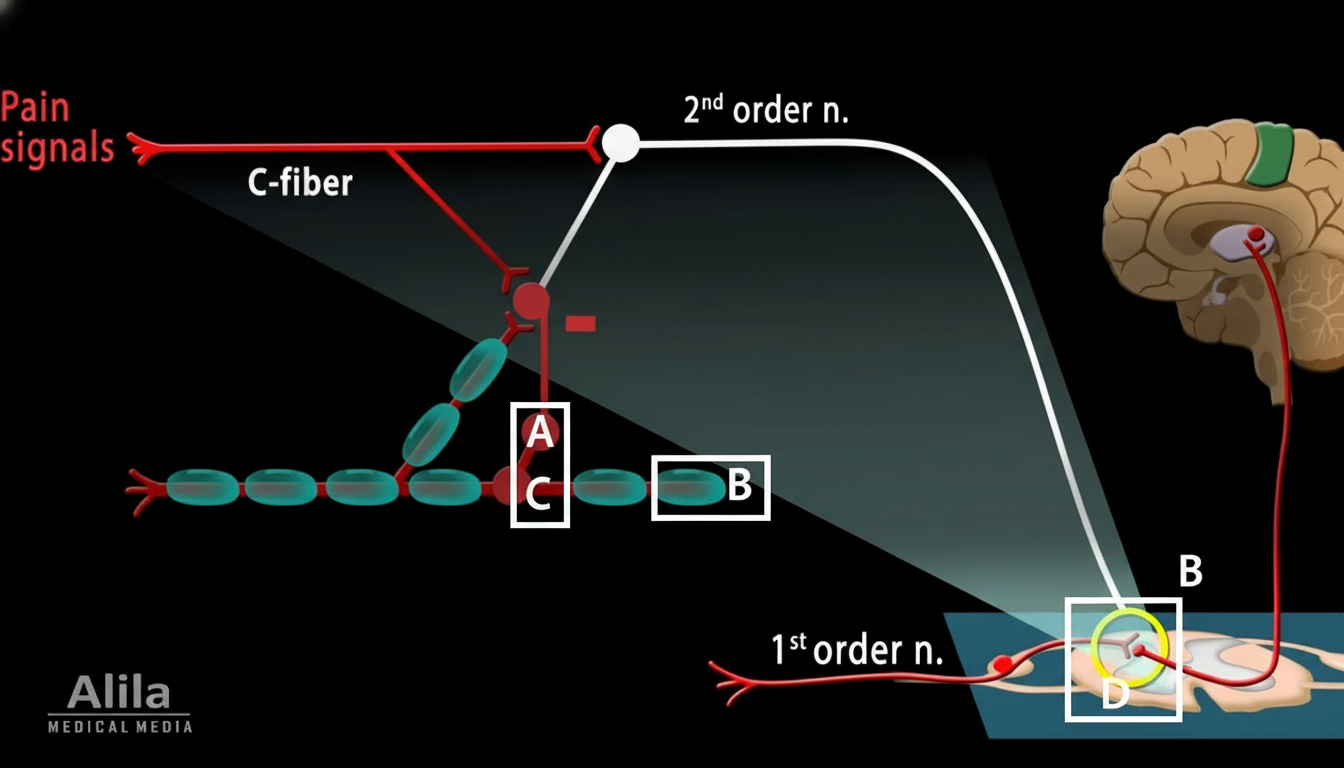
During massage, activation of large-diameter myelinated Aβ afferents helps close the pain gate by recruiting inhibitory interneurons in the dorsal horn. Which marked area is located on the myelin sheath of the large Aβ afferent shown in the diagram?
A physiology experiment is conducted in which a glass microelectrode is inserted into a Pacinian corpuscle to record receptor potentials during different levels of stimulation. Increasing stimulus strength from 10 percent of maximum to 30 percent of maximum causes a 40 percent increase in the amplitude of the receptor potential. Increasing the stimulus potential from 70 percent of maximum to 90 percent of maximum is most likely to cause what increase in the amplitude of the receptor potential (in percent)?
A 39-year-old neurosurgeon picks up a scalpel, which activates numerous sensory receptors in her hand. An increase in which of the following best describes the basis for transduction of the sensory stimuli into nerve impulses?
Which of the following activates vanilloid receptors in the urinary bladder?
Substance P is increased in response to pain in the periphery, mediated by which of the following?
Practice by Chapter
General Sensory Physiology
Practice Questions
Somatosensation
Practice Questions
Pain Physiology
Practice Questions
Vision and Optics
Practice Questions
Retinal Physiology
Practice Questions
Visual Pathways and Processing
Practice Questions
Auditory System
Practice Questions
Vestibular System
Practice Questions
Taste and Smell
Practice Questions
Sensory Integration
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app