
Sensory Systems — MCQs

On this page
Nerve endings sensitive to noxious stimuli are present in all except which of the following?
Reissner's membrane separates which of the following?
The highest degree of pain localization comes from which of the following?
Sound reaches maximum amplitude depending on its frequency at which structure?
Second order neurons in the optical pathway are present in which of the following structures?
What part of the retina provides the highest visual resolution?
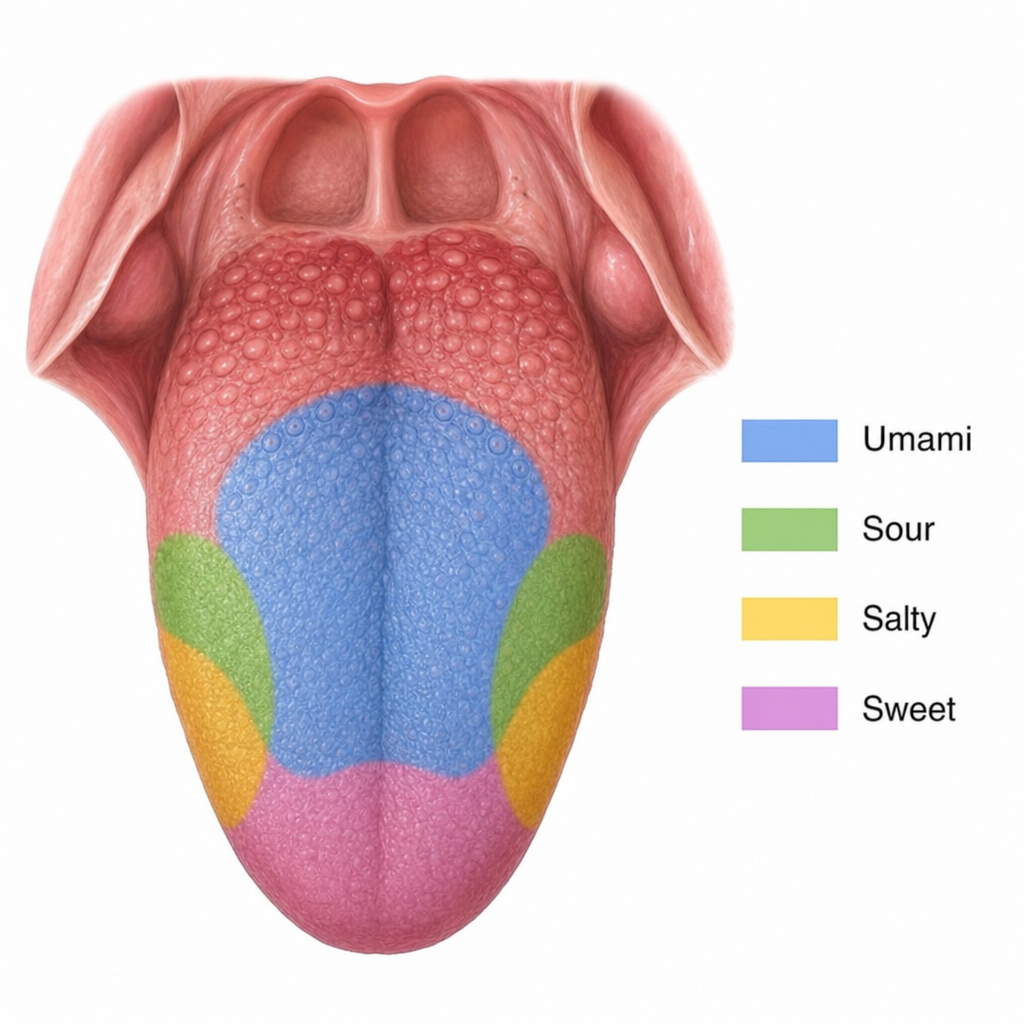
Which substance is responsible for the taste sensation marked in blue?
A lesion at which part of the visual pathway causes homonymous hemianopia?
Constriction of pupils is seen in:
Cerebrospinal fluid (CSF) is similar to which of the following fluids?
Practice by Chapter
General Sensory Physiology
Practice Questions
Somatosensation
Practice Questions
Pain Physiology
Practice Questions
Vision and Optics
Practice Questions
Retinal Physiology
Practice Questions
Visual Pathways and Processing
Practice Questions
Auditory System
Practice Questions
Vestibular System
Practice Questions
Taste and Smell
Practice Questions
Sensory Integration
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app