
Sensory Systems — MCQs

On this page
During the process of accommodation, there is a change in the shape of the lens. This change involves:
Hot water bottle relieves pain of abdominal spasm by:
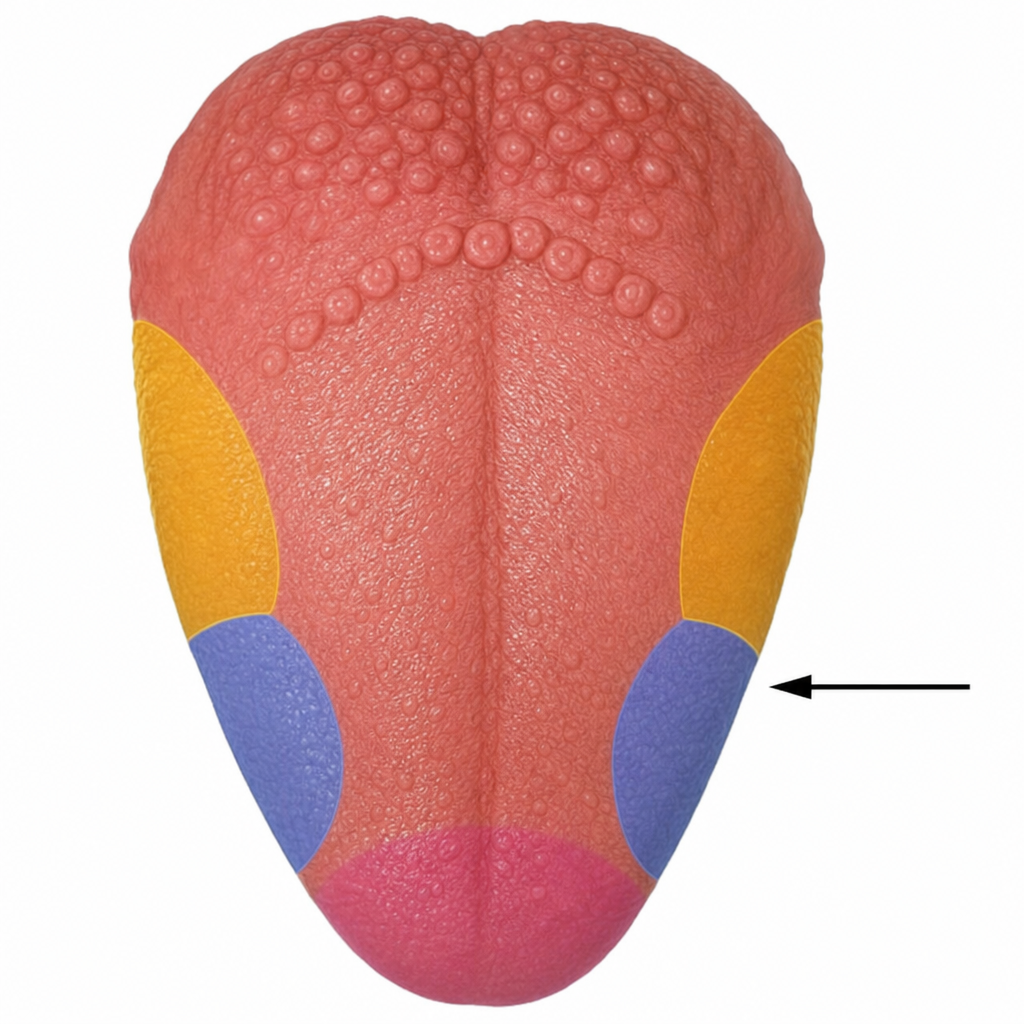
According to the historical, now-discredited tongue map, the indicated area was associated with which taste?
Which sensory receptor is primarily responsible for mediating slow vibration sensation?
Primary afferent fibers secrete which nociceptive substance at the dorsal horn?
Which of the following is true during far accommodation of the eyes?
Which of the following best describes the permeability to sodium and potassium in rod cells in response to light?
Impulses generated in the taste buds of the tongue reach the cerebral cortex via the
Function of the ossicles in the middle ear is to
Retinal cells which secrete acetylcholine are:
Practice by Chapter
General Sensory Physiology
Practice Questions
Somatosensation
Practice Questions
Pain Physiology
Practice Questions
Vision and Optics
Practice Questions
Retinal Physiology
Practice Questions
Visual Pathways and Processing
Practice Questions
Auditory System
Practice Questions
Vestibular System
Practice Questions
Taste and Smell
Practice Questions
Sensory Integration
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app