
Sensory Systems — MCQs

On this page
What is the function of utricle and saccule?
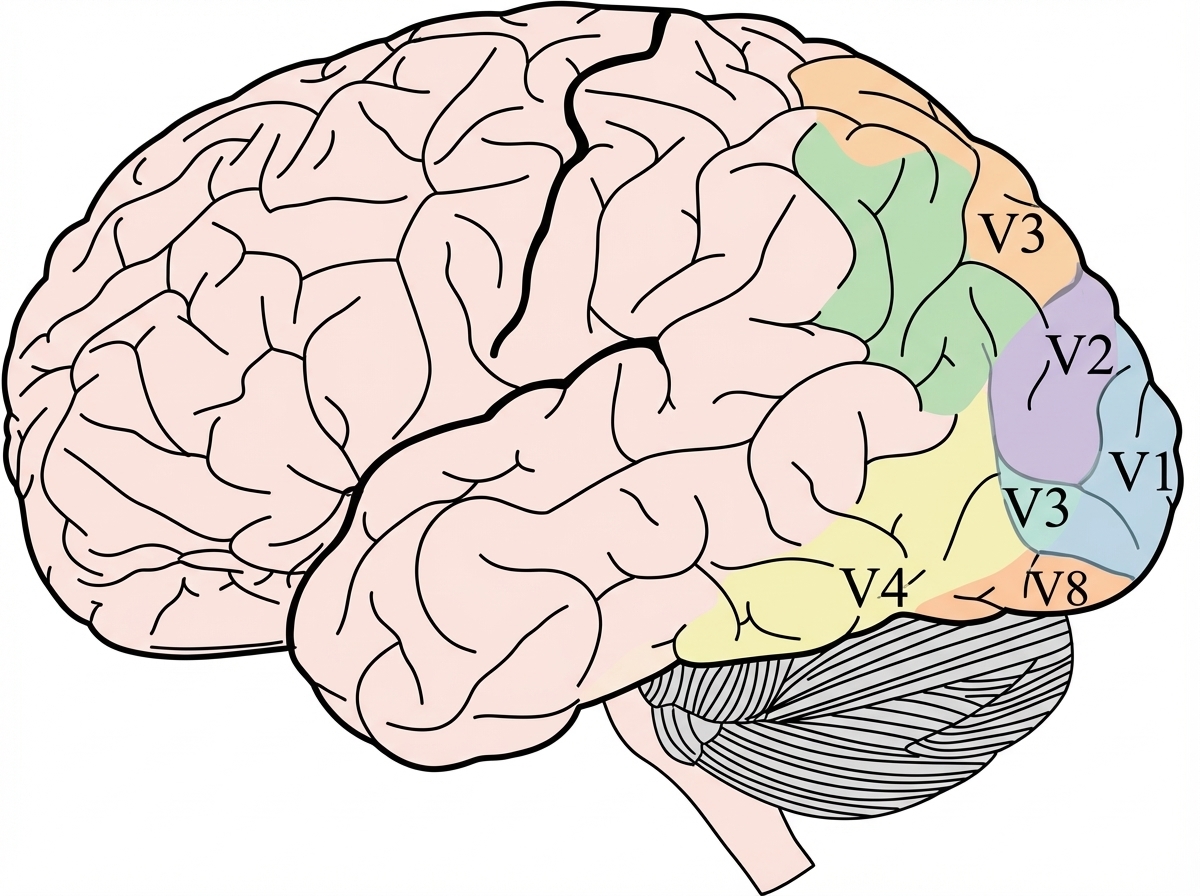
Which of the following higher visual areas is most specifically associated with the proposed color-selective processing distinct from the established V4 color processing area?
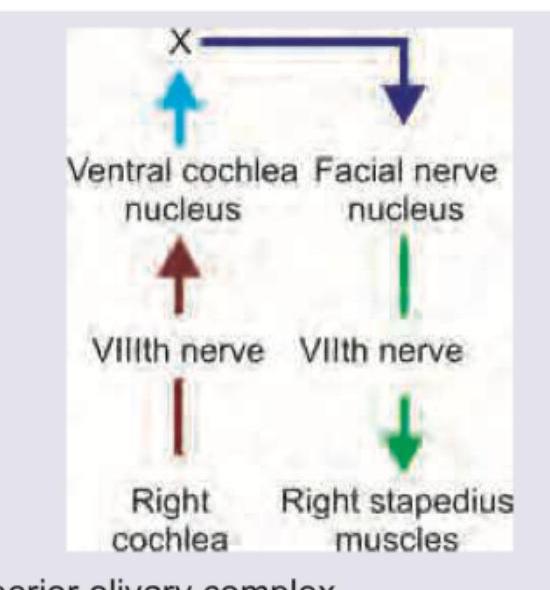
The image given below shows stapedial reflex. What does ' $X$ ' denote?
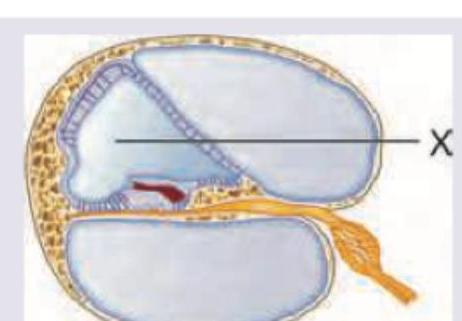
What is correct about the composition of fluid in the area marked as X?
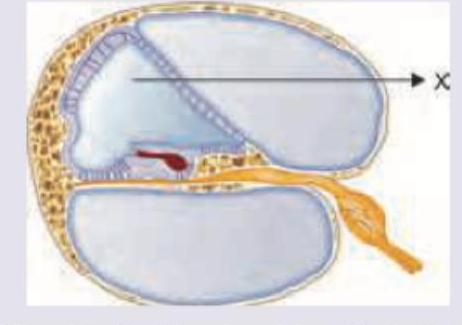
What is correct about the composition of fluid in the area marked as $X$ ?
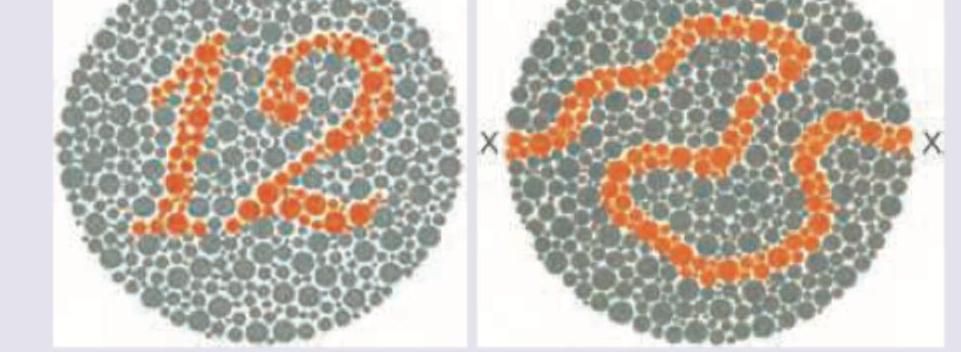
Which of the following cells in the brain predominantly convey the high-spatial-resolution and red-green chromatic information through the parvocellular visual pathway needed to interpret the slide below? (Recent NEET Pattern 2016-17)
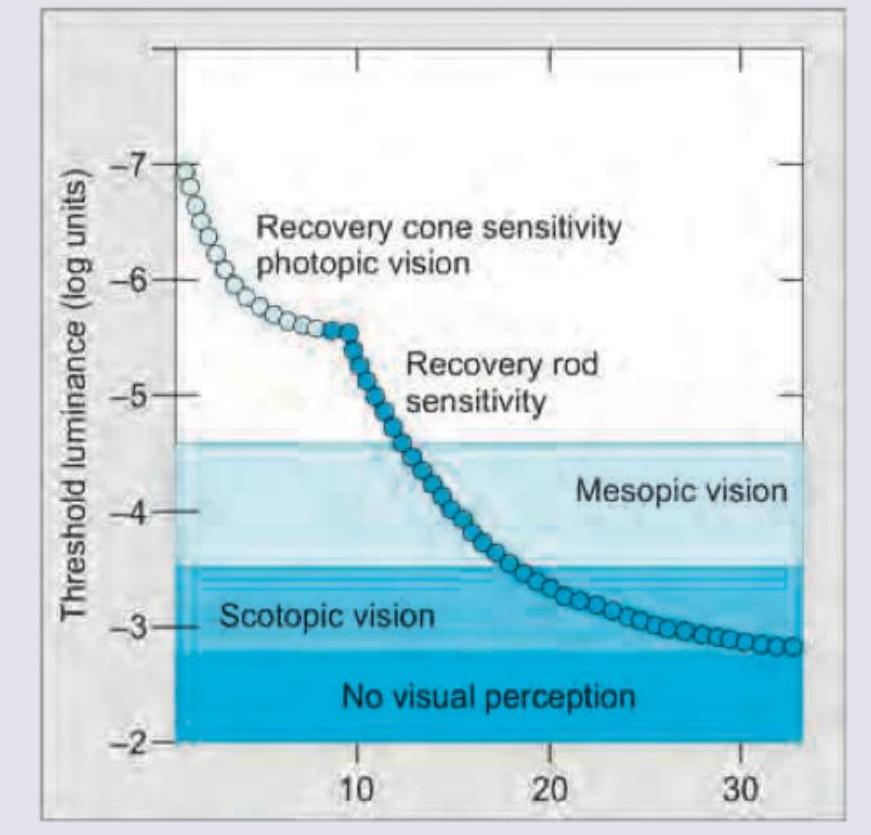
The image given below shows:
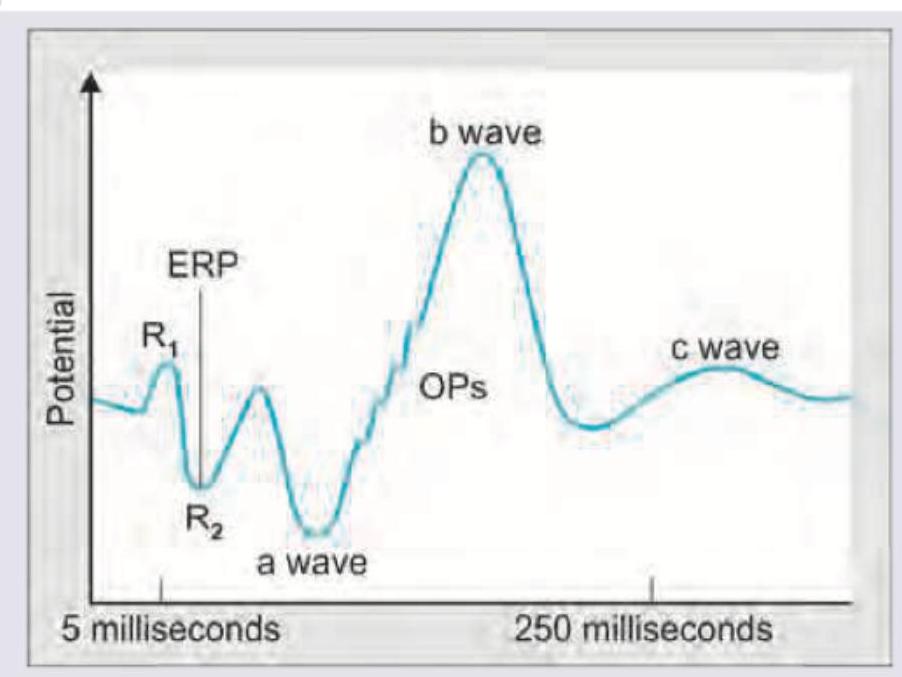
All are true about the recording shown except:
A woman suffered a sunburn while enjoying a vacation on the beach. Now, while taking a shower, the lukewarm water (40° C) touching her back caused her to feel pain. What types of receptors were activated by the lukewarm water, and why did she experience pain?
Select the correct option regarding the function of receptors:
Practice by Chapter
General Sensory Physiology
Practice Questions
Somatosensation
Practice Questions
Pain Physiology
Practice Questions
Vision and Optics
Practice Questions
Retinal Physiology
Practice Questions
Visual Pathways and Processing
Practice Questions
Auditory System
Practice Questions
Vestibular System
Practice Questions
Taste and Smell
Practice Questions
Sensory Integration
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app