
Respiratory System — MCQs

On this page
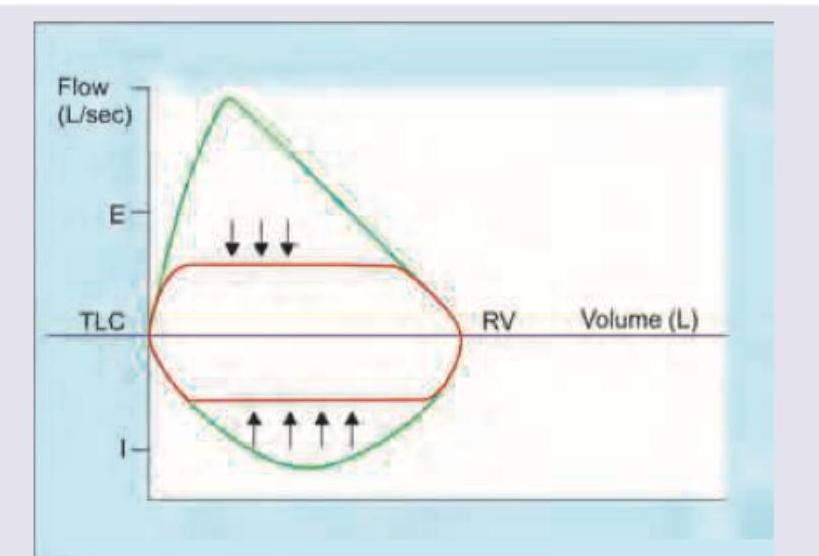
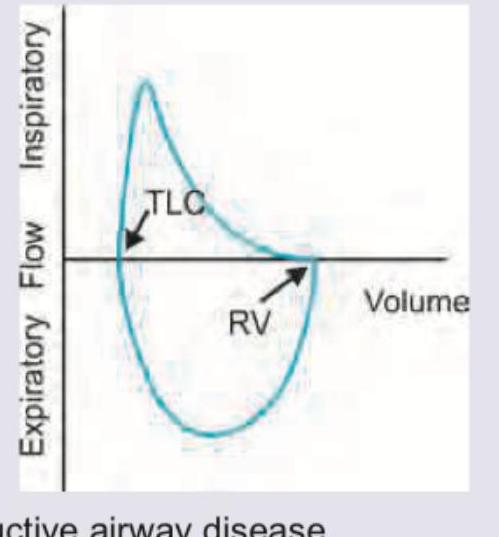
Which flow volume curve recording is shown below?
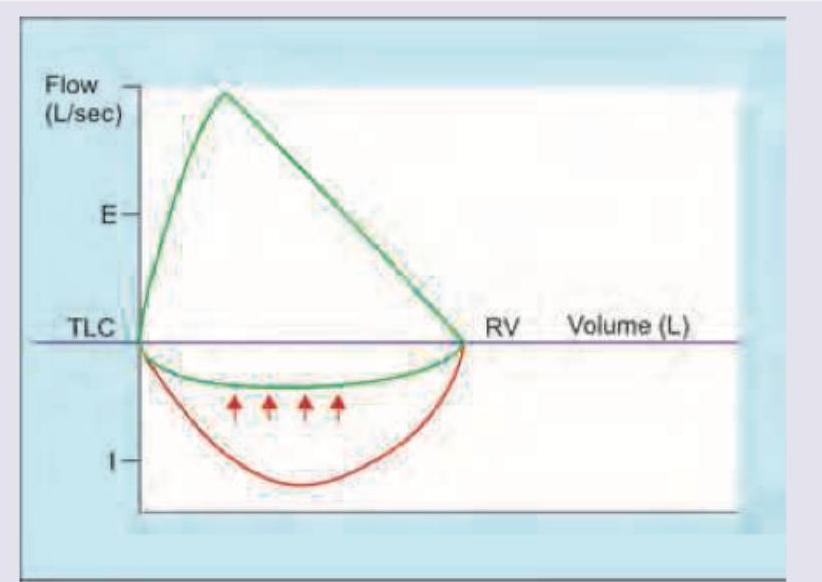
Which flow volume curve recording is shown below?
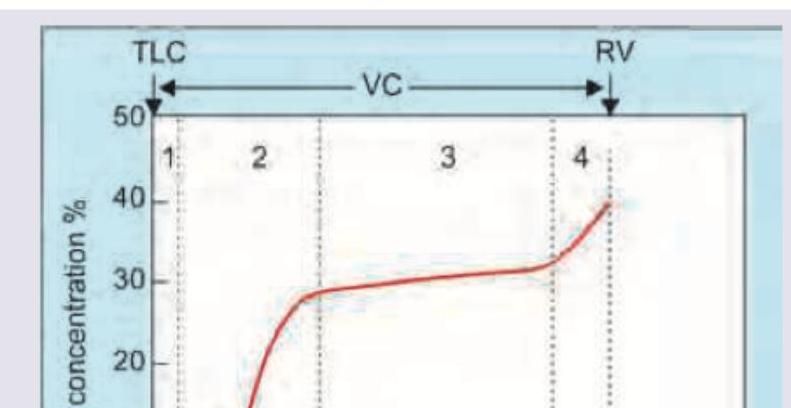
Which of the following areas of nitrogen washout test indicate closing volume?
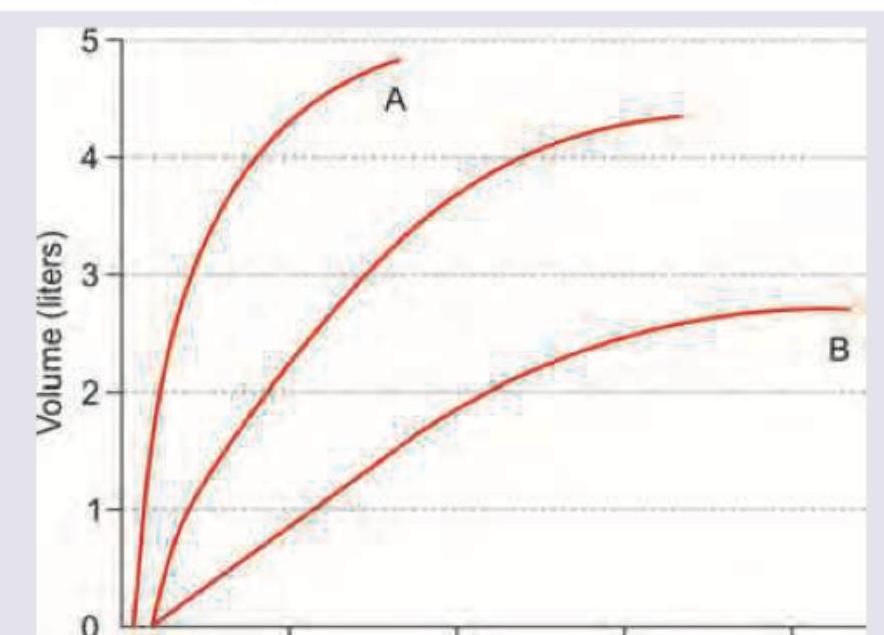
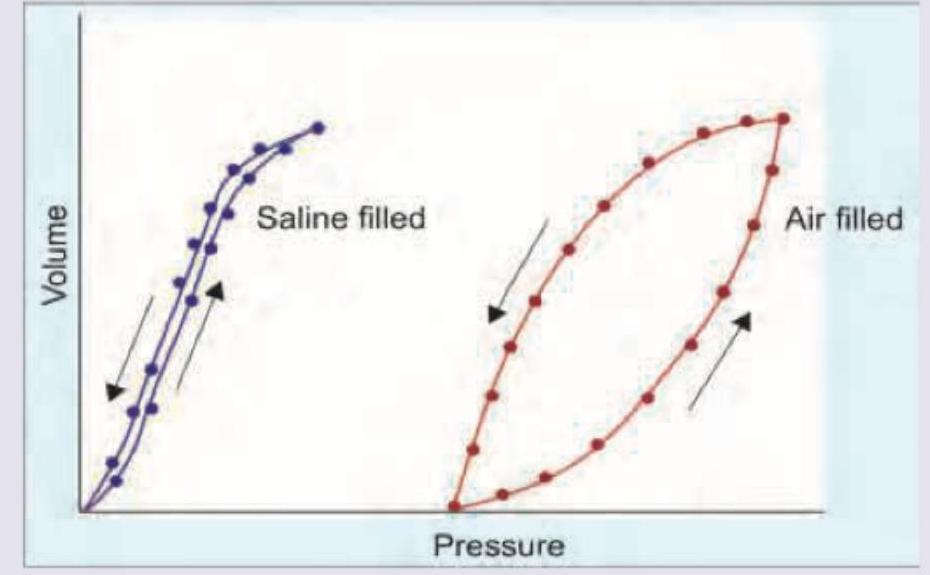
Which statement related to lung compliance shown in the image below is correct:
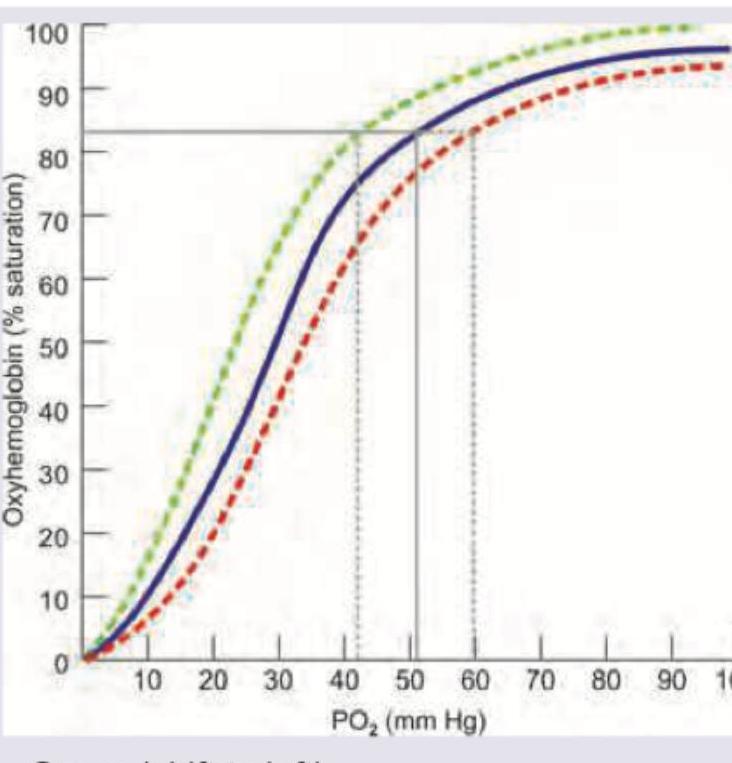
The baseline oxyhemoglobin dissociation curve is depicted in blue color. Shift of curve to which side indicates Bohr effect?
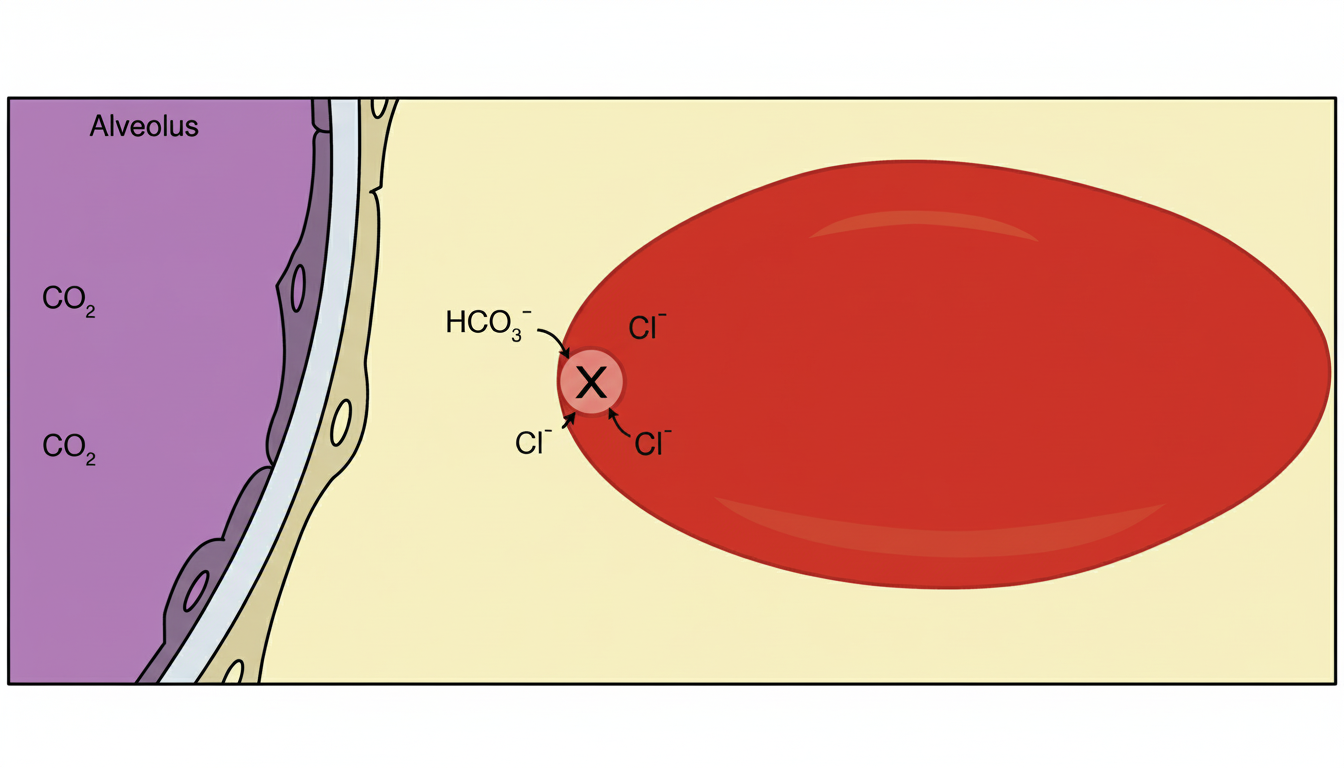
Which protein is responsible for the effect shown in RBC marked as $X$ ?
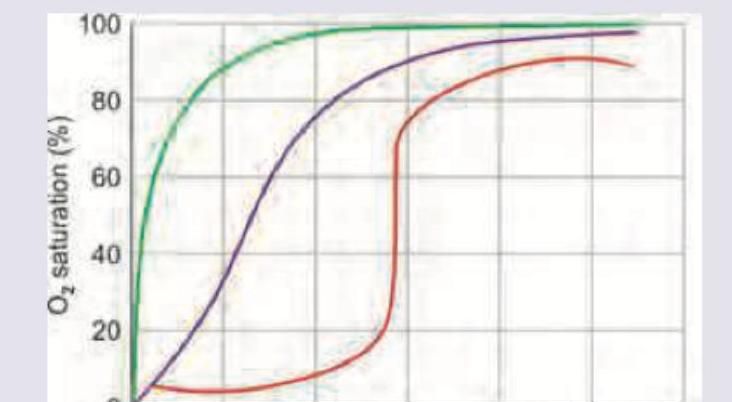
Which of the following dissociation curve mentioned is for myoglobin?
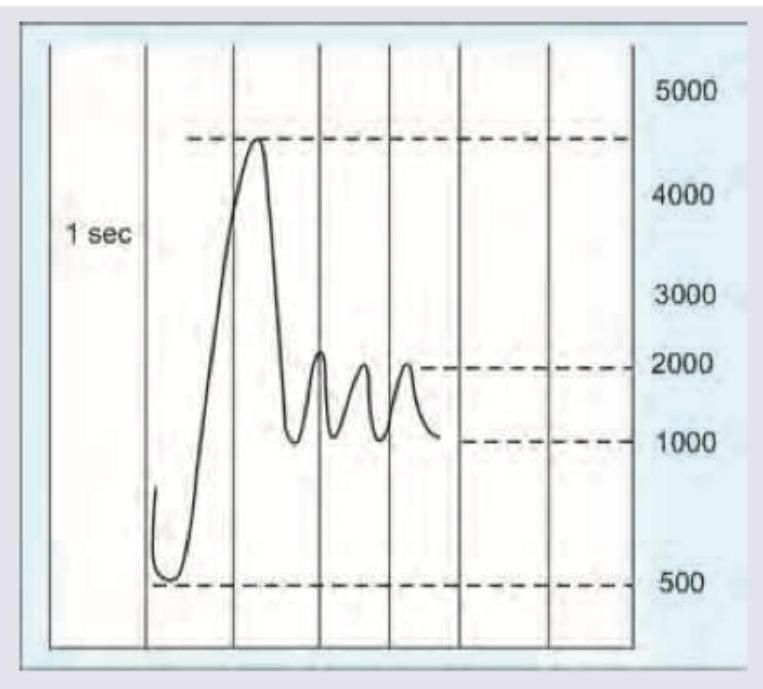
Calculate the FEV1/FVC ratio from the spirometry reading shown below.
Hysteresis is observed between the deflation and inflation curves in an isolated lung compliance diagram. What is the best description for the same?
Which of the following pattern is reflected in the flow-volume curve?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app