
Respiratory System — MCQs

On this page
Activation of which receptor causes pulmonary vasoconstriction?
What causes effort during normal respiration?
The oxygen-hemoglobin dissociation curve is shifted to the left by:
Anemic hypoxia is seen in which of the following conditions?
Least arteriovenous oxygen difference is seen in which of the following conditions?
Death due to cyanide poisoning results from which of the following types of anoxia?
The Hb-O2 dissociation curve is shifted to the left by which of the following?
Which of the following changes does NOT occur in the blood as it passes through the systemic capillaries?
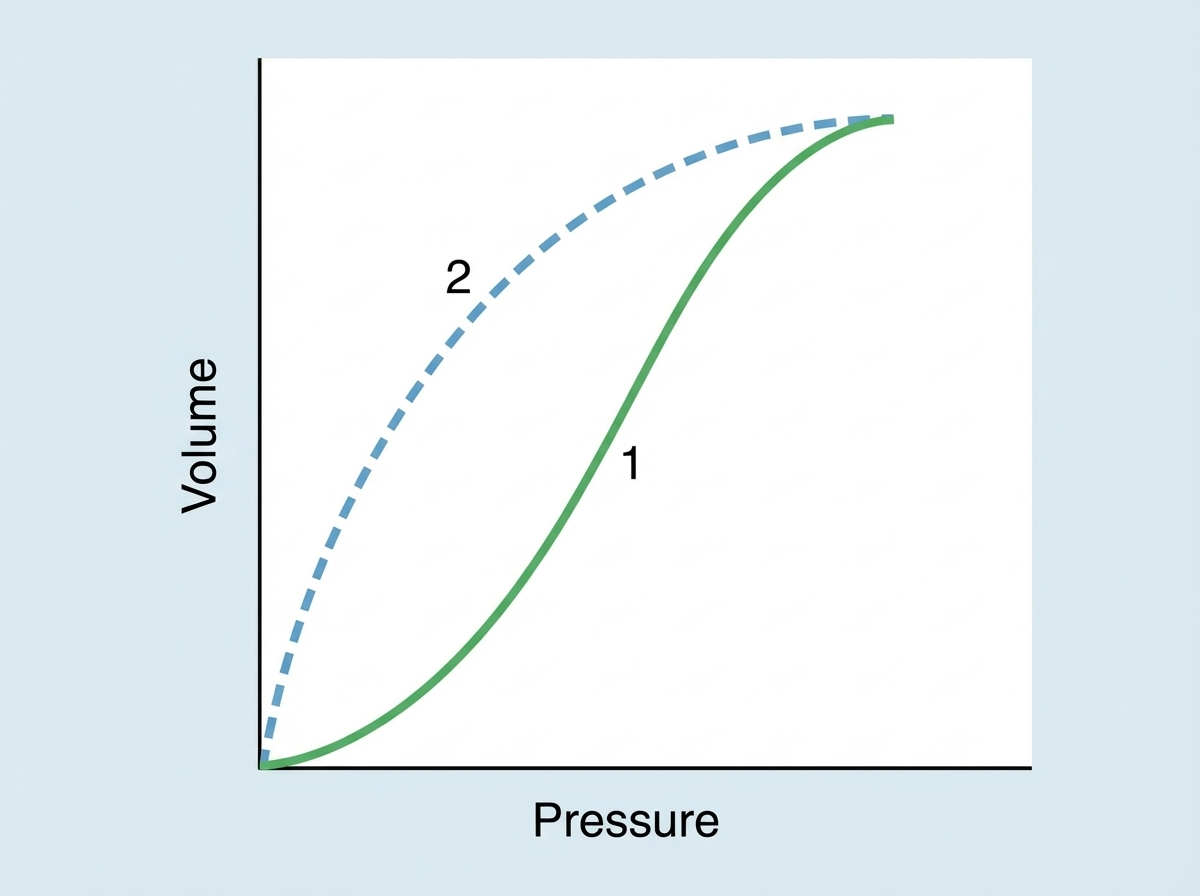
Identify the process indicated by '1' in the illustration depicting lung compliance.
The alveoli are normally kept dry by which of the following mechanisms?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app