
Respiratory System — MCQs

On this page
True regarding vascularity of the lung is:
How is the volume of inspired air that actually ventilates the alveoli calculated?
What is the most important stimulus controlling the level of resting ventilation?
Oxygen delivery to tissues is decreased by:
Lung compliance is increased in which of the following conditions?
Cyanosis does not occur in severe anaemia because:
What is the formula for transthoracic compliance?
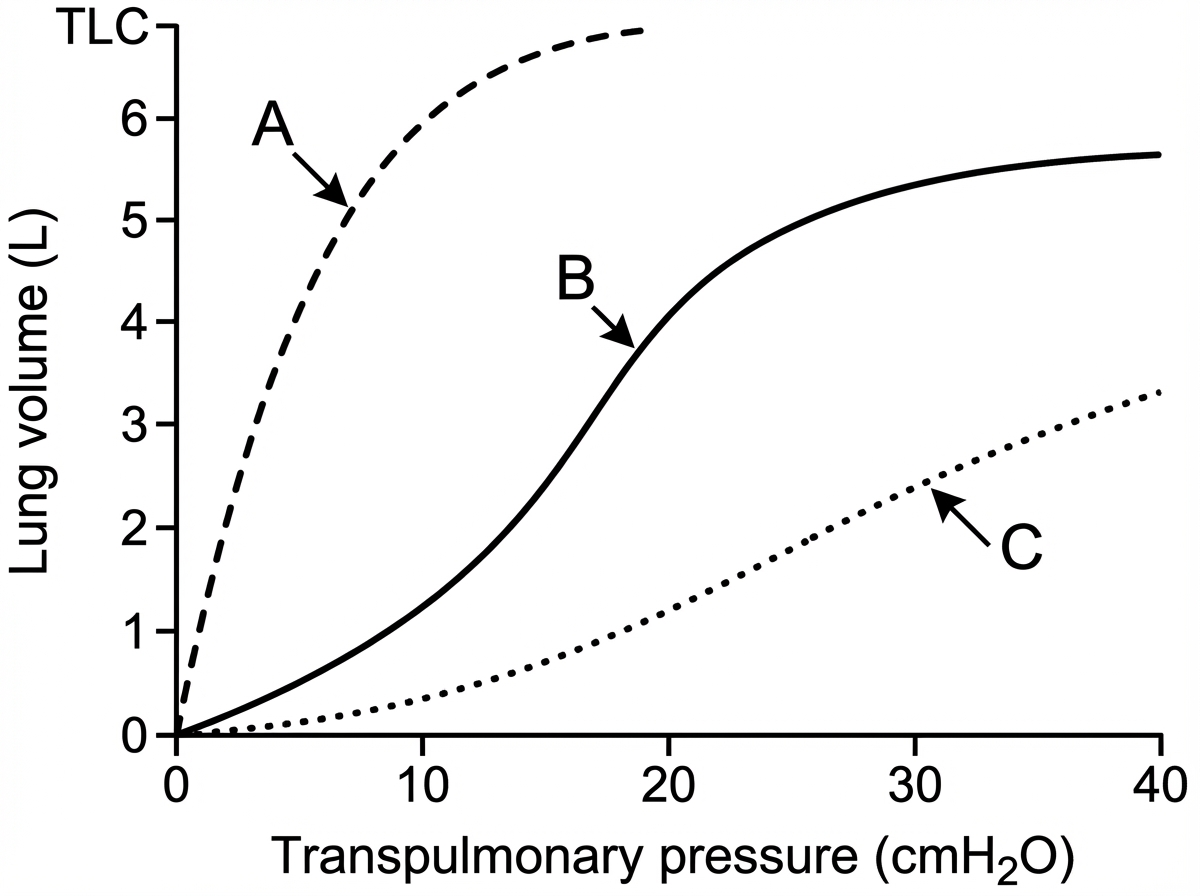
Curve A signifies which of the following?
What type of blood flow is typically seen in the apex of the lung?
Which of the following will not cause a low lung diffusing capacity (DL)?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app