
Respiratory System — MCQs

On this page
The initiation of the first breath in a newborn is due to changes in which of the following parameters?
Arrange the following physiological events in the sequence that occurs on exposure to hypoxia:
A 56-year-old woman with a 75-pack-year history of smoking cigarettes presents with shortness of breath. Pulmonary function tests revealed the following: Functional residual capacity 4.5L, Inspiratory reserve volume 1.5L, Inspiratory capacity 2.0L, Vital capacity 3.0L. What is the residual volume of this patient?
Spirometry can measure which of the following lung volumes or capacities?
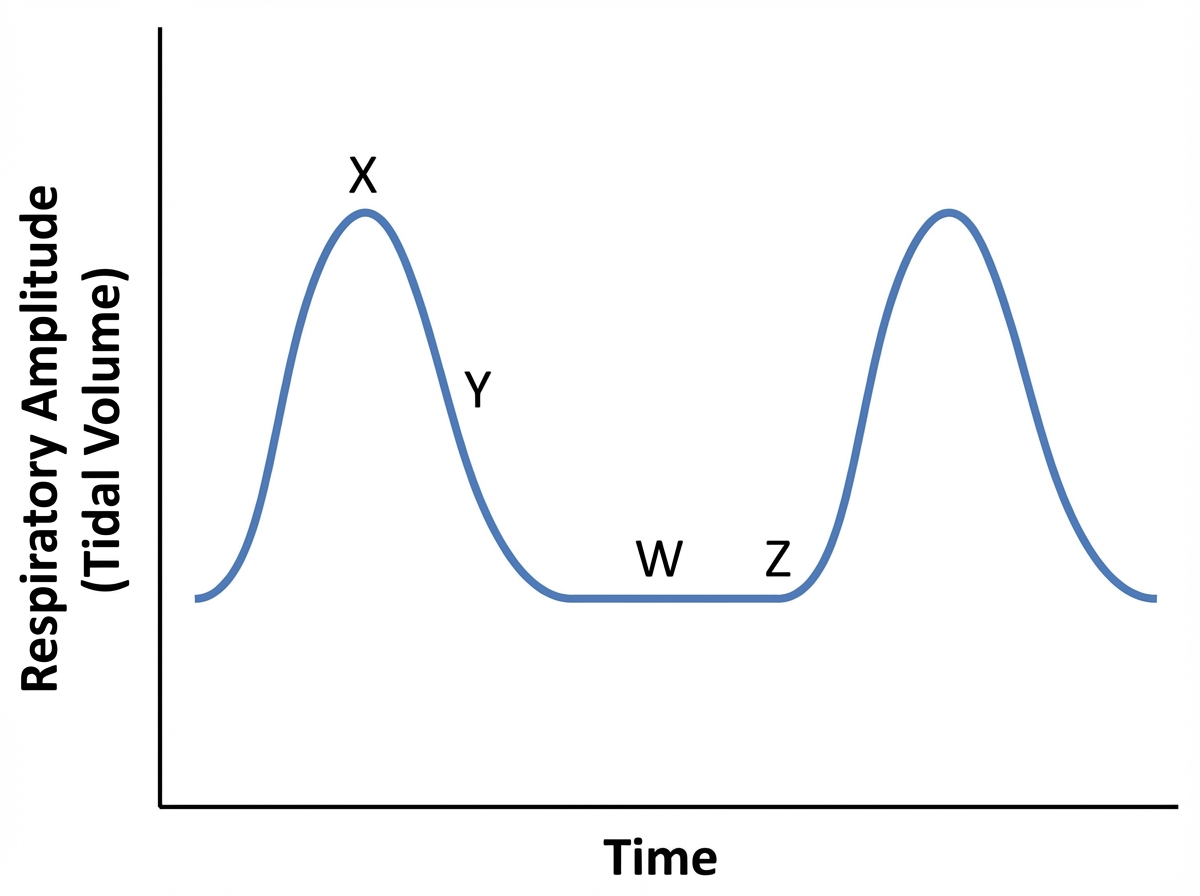
Which time point on the Cheyne-Stokes breathing graph is associated with the highest pCO2 of pulmonary arterial blood?
Oxygen therapy is least useful in which of the following conditions?
What is the key factor in the transport of carbon dioxide as bicarbonate?
Following birth, which of the following changes occur in the fetus?
Apneusis occurs when transection is at which level?
Which of the following statements are true about interstitial fibrosis?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app