
Respiratory System — MCQs

On this page
Moderate exercise is one of the most powerful stimulators of ventilation. By what mechanism does this occur?
The surfactant is produced by which of the following cells?
A 54-year-old man sustains third degree burns in a house fire. His respiratory rate is 30/min, Hb = 17 g/dL, arterial PO2 is 95 mm Hg, and arterial O2 saturation is 50%. What is the most likely cause of his low oxygen saturation?
What is the respiratory quotient of protein in the body?
Which of the following findings demonstrates a difference between pulmonary circulation and systemic circulation?
Diffusion of oxygen at the tissue level is affected in all the following poisoning except?
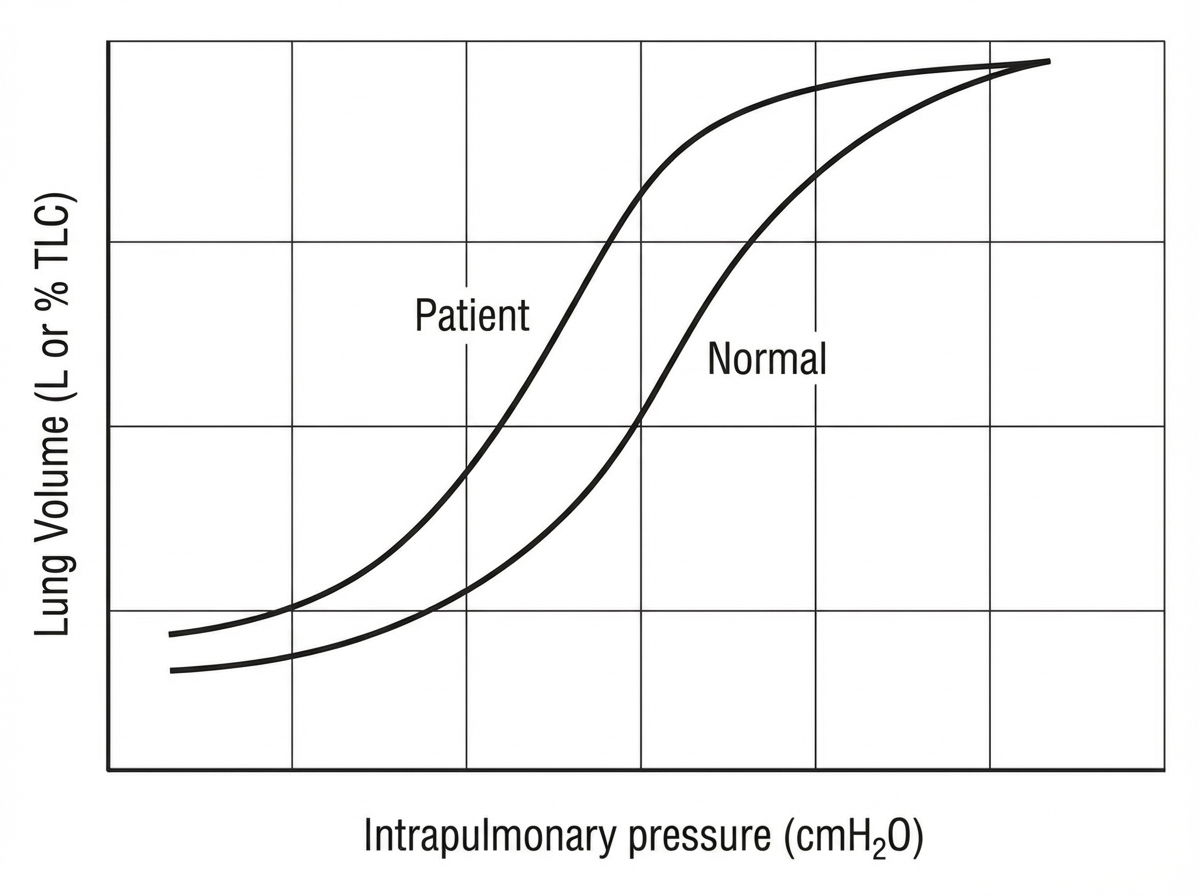
The provided pressure-volume curves represent a normal subject and a patient with a pulmonary disease. Based on these curves, what is the likely pulmonary condition of the patient?
CO2 retention is seen in which of the following conditions?
Closing volume is the volume of lung
Severe pulmonary congestion and edema is seen when PCWP rises above which value?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app