
Respiratory System — MCQs

On this page
Which of the following is NOT a cause of a rightward shift of the oxygen-hemoglobin dissociation curve?
Haemoglobin is the major buffer in blood. Bicarbonate ions diffuse out of erythrocytes into plasma in exchange for which ion?
In the ventilation-perfusion (V/Q) ratio curve for the normal lung, if the V/Q ratio is decreased, what will be the effect on pCO2 and pO2?
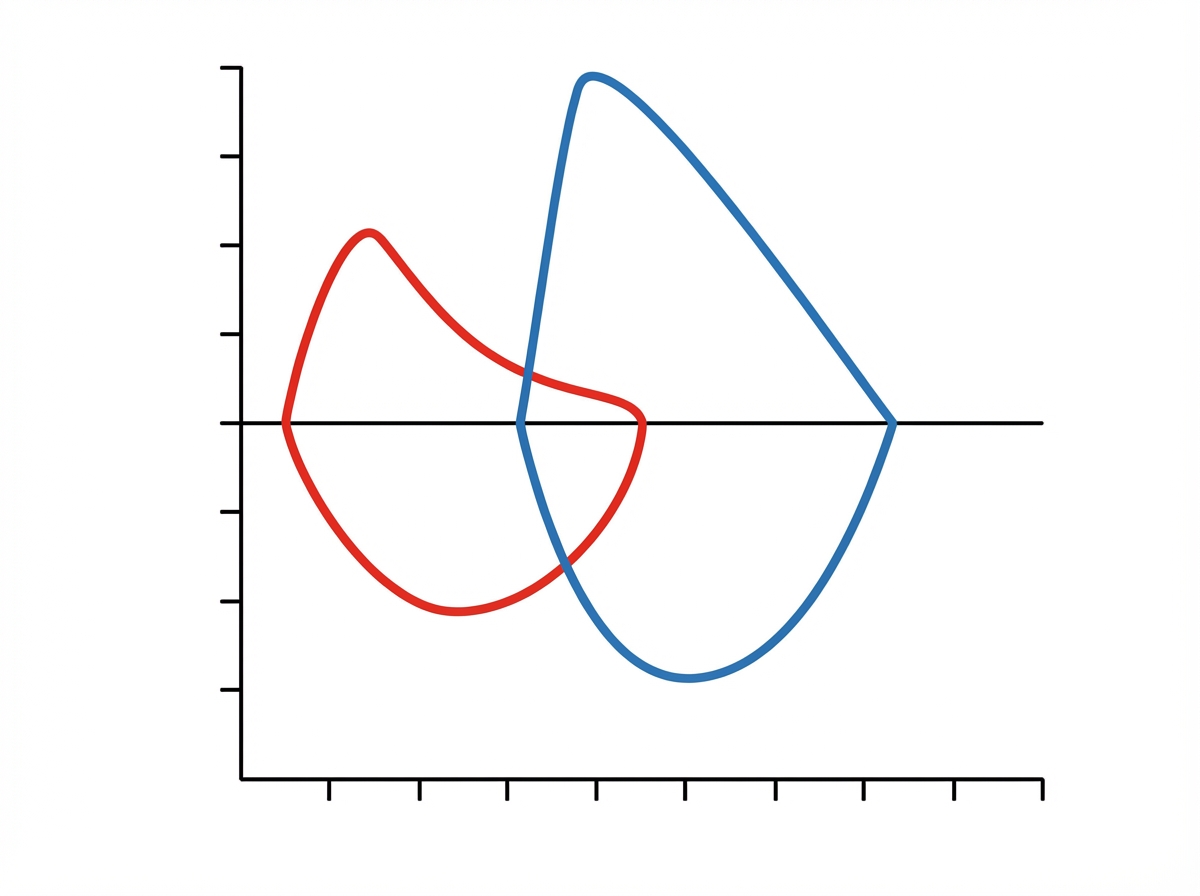
The given graph (x-axis: volume; y-axis: flow rate; blue loop: predicted normal; red loop: patient) likely depicts which of the following conditions, each of which is the only listed condition expected to produce the depicted obstructive pattern?
What causes the difference in the trajectory between the inspiratory loop and the expiratory loop in a flow-volume curve?
Pulmonary vasoconstriction is caused by:
Which of the following statements is FALSE regarding the oxygen dissociation curve?
The shift of the oxygen dissociation curve to the left is facilitated by all except?
Routine spirometry cannot estimate which of the following lung volumes or capacities?
What is the haemoglobin derivative formed due to the reaction of CO2 with blood?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app