
Respiratory System — MCQs

On this page
One gram of hemoglobin, when fully saturated in arterial blood, carries what volume of oxygen?
Cyanosis may be seen in which of the following types of hypoxia?
All of the following lead to increased dissociation of O2 from Hb except?
In a man weighing 200 pounds, what is the approximate volume of his anatomic dead space?
Calculate the alveolar ventilation per minute of a patient with a respiratory rate of 14/min and a tidal volume of 500 ml.
Lung compliance is defined as:
Higher hematocrit in venous blood than in arterial blood is due to which of the following?
A patient presents with a right-to-left shunt. The oxygen content in the arterial and venous blood is 18 ml/100 ml and 14 ml/100 ml, respectively. The oxygen content at the pulmonary capillary is 20 ml/100 ml. What is the percentage of shunting of cardiac output?
With respect to oxygen and carbon dioxide transport in the blood, which of the following statements is correct?
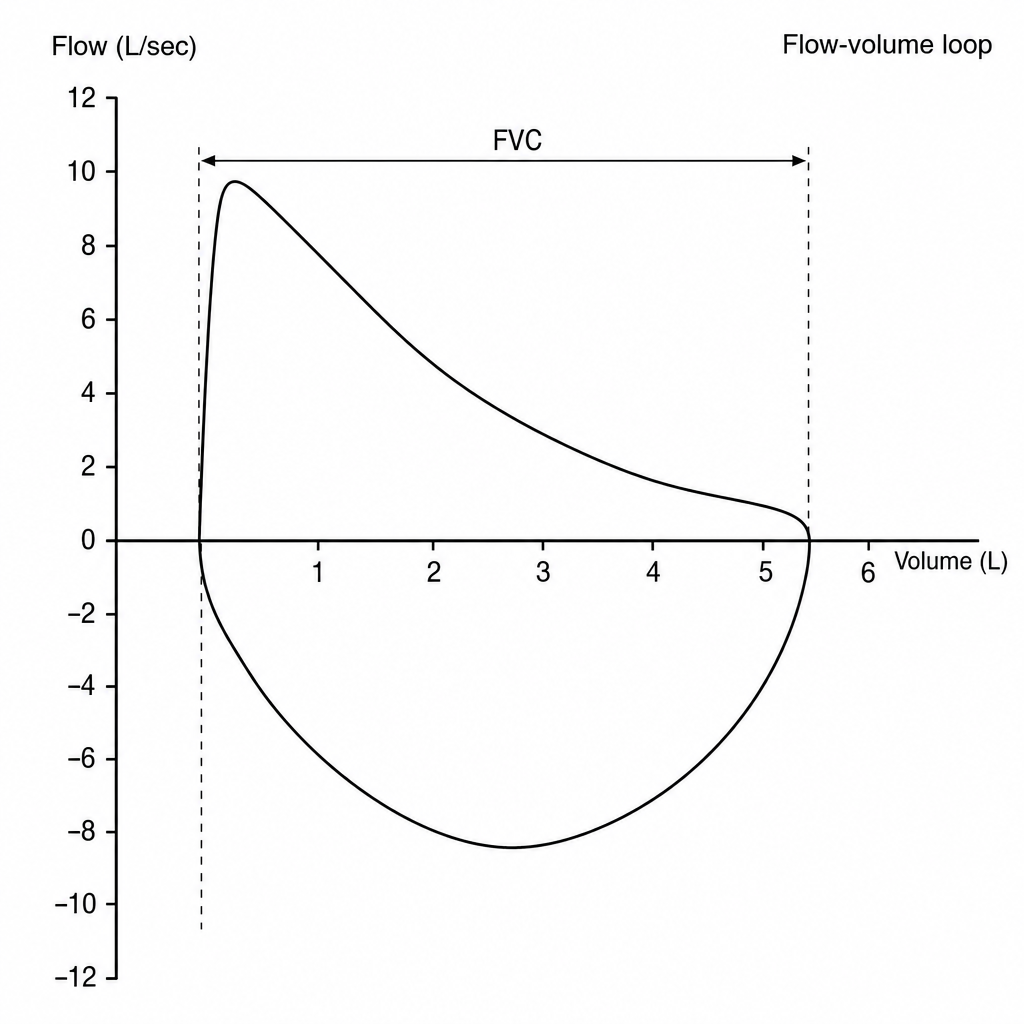
In the expiratory flow volume loop shown below, what is the forced vital capacity?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app