
Respiratory System — MCQs

On this page
Medullary chemoreceptors are primarily sensitive to which of the following?
What is the normal partial pressure of carbon dioxide (pCO2) in exhaled air?
Decreased O2 affinity of Hb in blood with decreased pH is known as which effect?
Oxygen release to tissues is affected by all of the following EXCEPT:
Regarding lung volumes, which of the following is true?
Oxygen affinity of hemoglobin increases with which of the following?
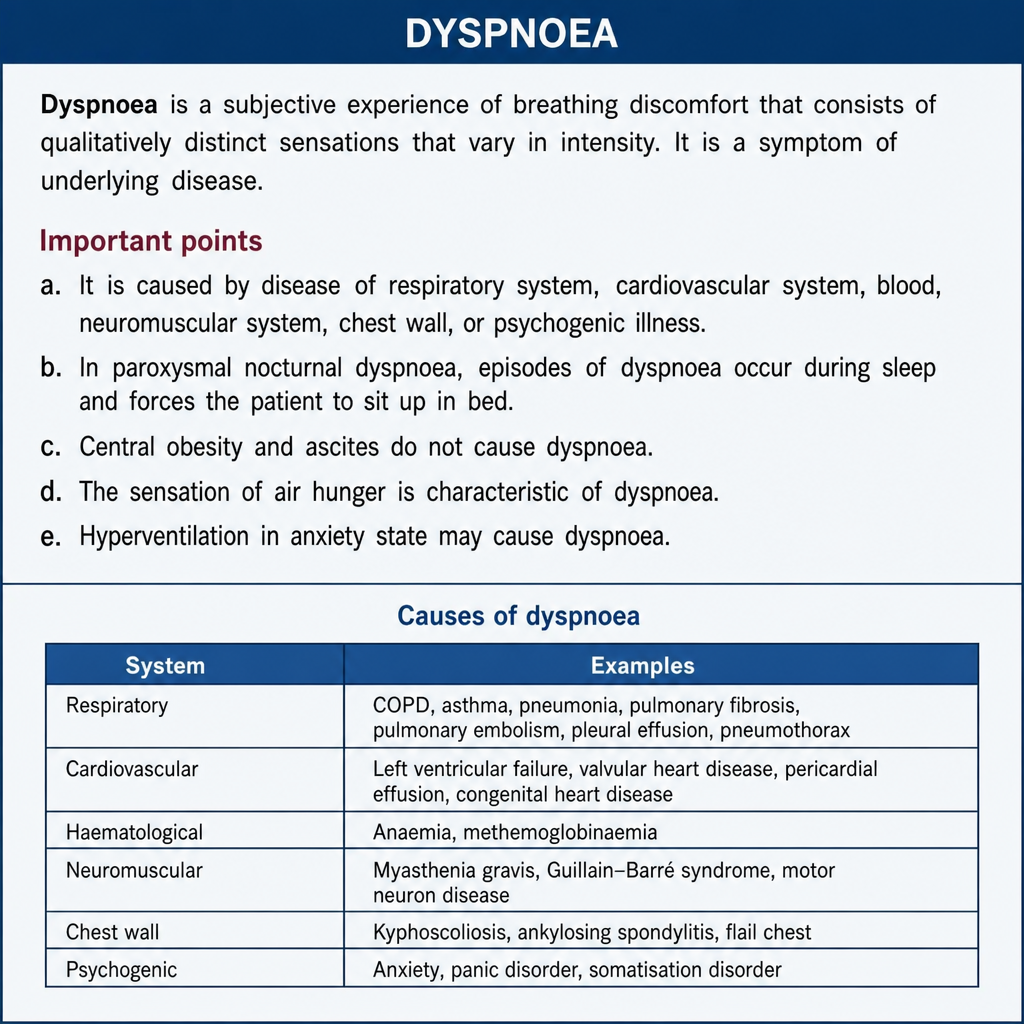
Which of the following statements regarding dyspnoea are True or False?
PO2 is maximum in which part of the lung?
With each quiet inspired breath, what fraction of alveolar air is replaced?
A 49-year-old man has a pulmonary embolism that completely blocks blood flow to his left lung. As a result, which of the following will occur?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app