
Respiratory System — MCQs

On this page
What is the volume of air taken into the lungs during normal respiration called?
Which hormone accelerates surfactant production?
Which of the following is not a consequence of stimulation of lung C fiber endings?
What is the reason for the sigmoid shape of the hemoglobin-oxygen dissociation curve?
An anesthetized patient is mechanically ventilated at her normal tidal volume but at twice her normal frequency. When mechanical ventilation is stopped, the patient fails to breathe spontaneously for 1 minute. This temporary cessation of breathing occurs because:
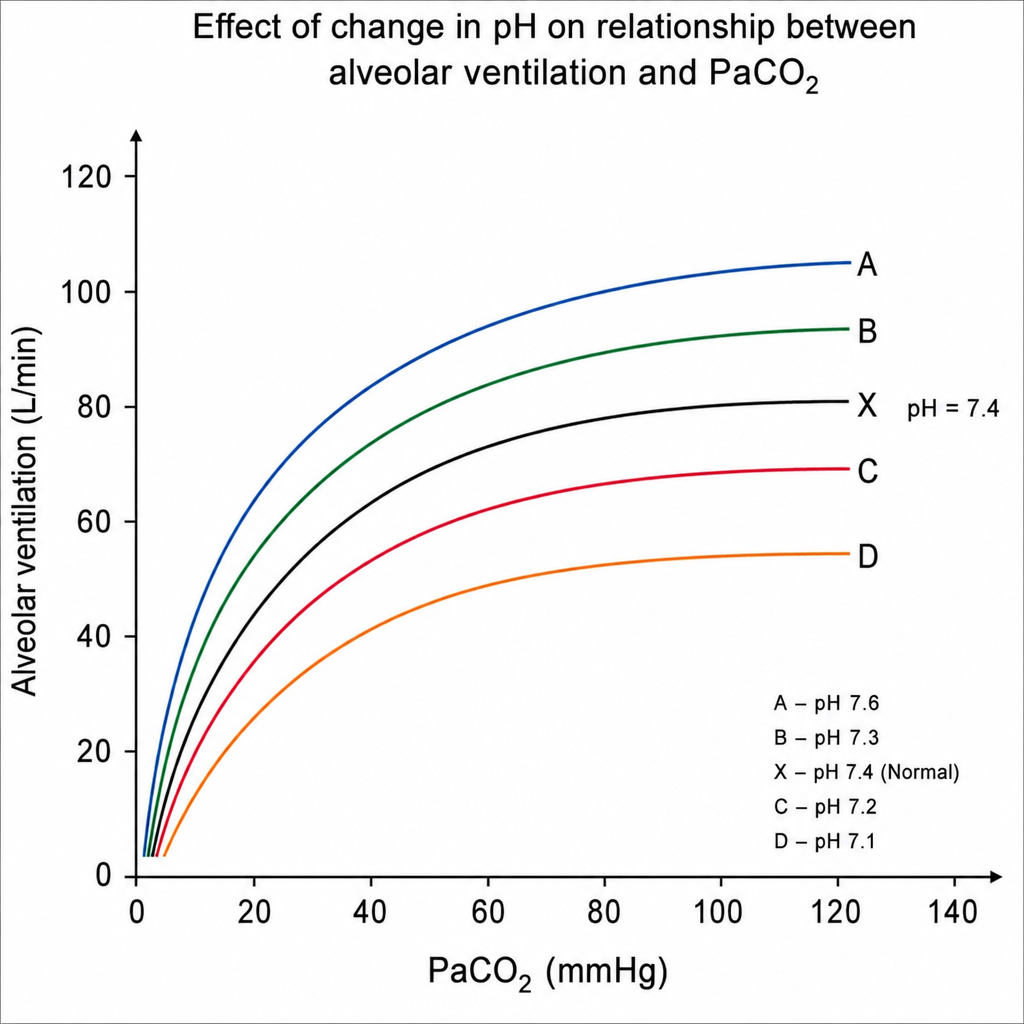
In the following diagram, curve X represents the normal relationship between alveolar ventilation and PaCO2 when PaO2 is 100 mmHg. If pH decreases from 7.4 to 7.3, to which curve will the relationship shift?
What is true regarding the alveolar-arterial oxygen gradient (A-a gradient)?
Under resting conditions, what is the total body oxygen consumption?
Apneusis occurs when there is damage to:
Which of the following is a typical manifestation of chronic hyperventilation?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app