
Respiratory System — MCQs

On this page
Which of the following best characterizes the pulmonary circulation?
Arterial PO2 is decreased in hypoxia due to which of the following conditions?
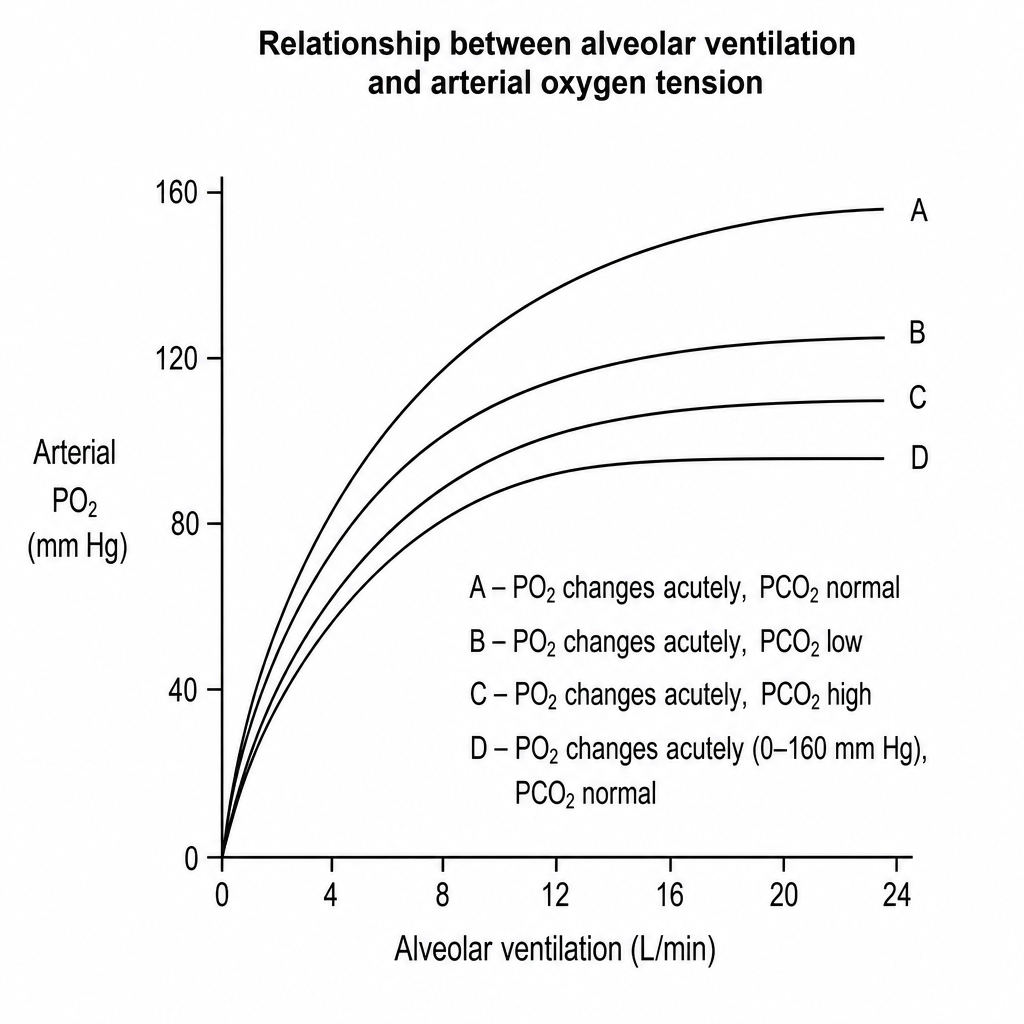
The following set of diagrams show the relationship between alveolar ventilation and arterial oxygen tension. Which diagram describes the situation when pO2 changes acutely over a range of 0-160 mm Hg, while pCO2 remains normal?
The functional residual capacity is best defined as the sum of which two lung volumes?
Dead space is increased by all, except:
The oxygen buffer function of hemoglobin is related to which of the following?
Which spirometry feature is characteristic of asthma?
Conversion of angiotensin-I to angiotensin-II occurs in which organ?
Which reflex is associated with hyperinflation of the lung?
Which of the following factors does NOT cause a rightward shift of the oxygen-hemoglobin dissociation curve?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app