
Respiratory System — MCQs

On this page
Which of the following physiological conditions will lead to pulmonary vasodilation?
At which point is the concentration of CO2 the least?
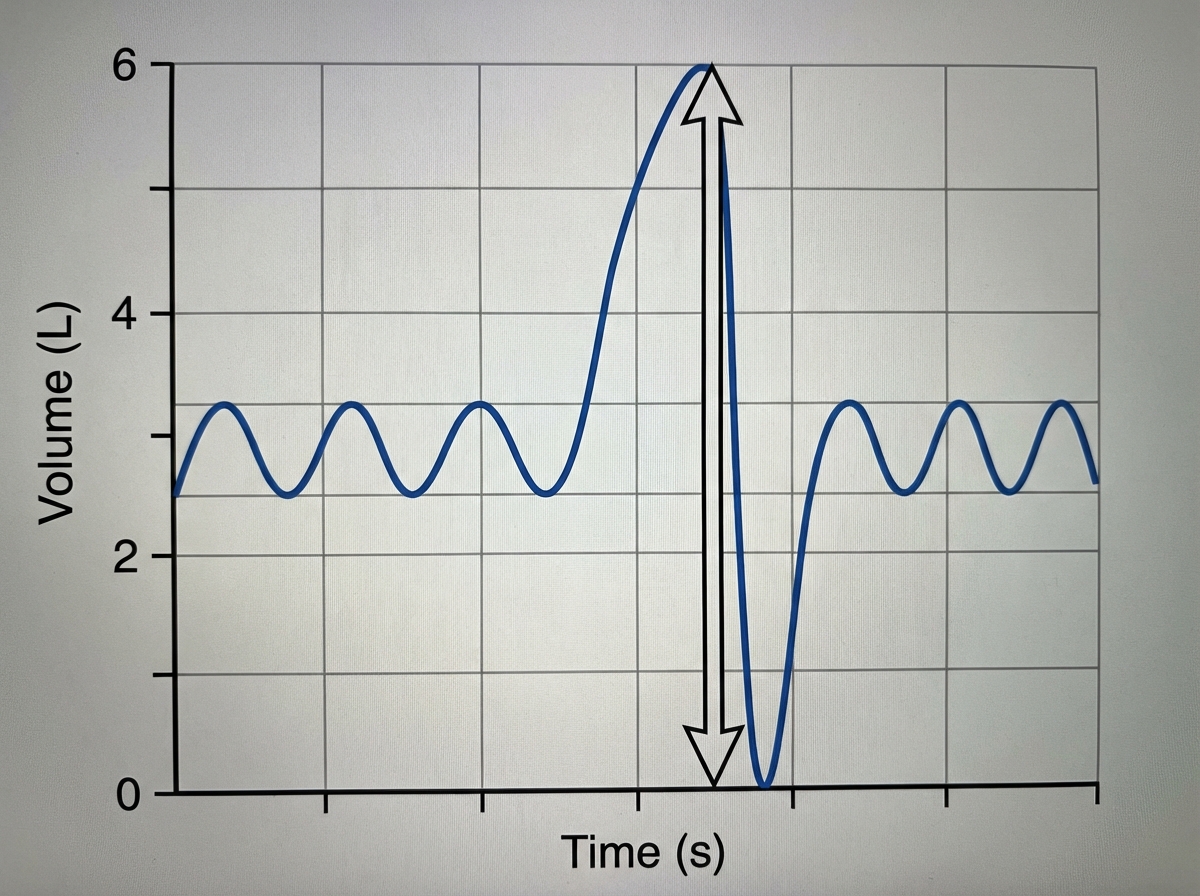
The following illustration of the Spirogram showing the arrow indicates:
Which is responsible for respiratory drive?
Tidal volume is calculated by?
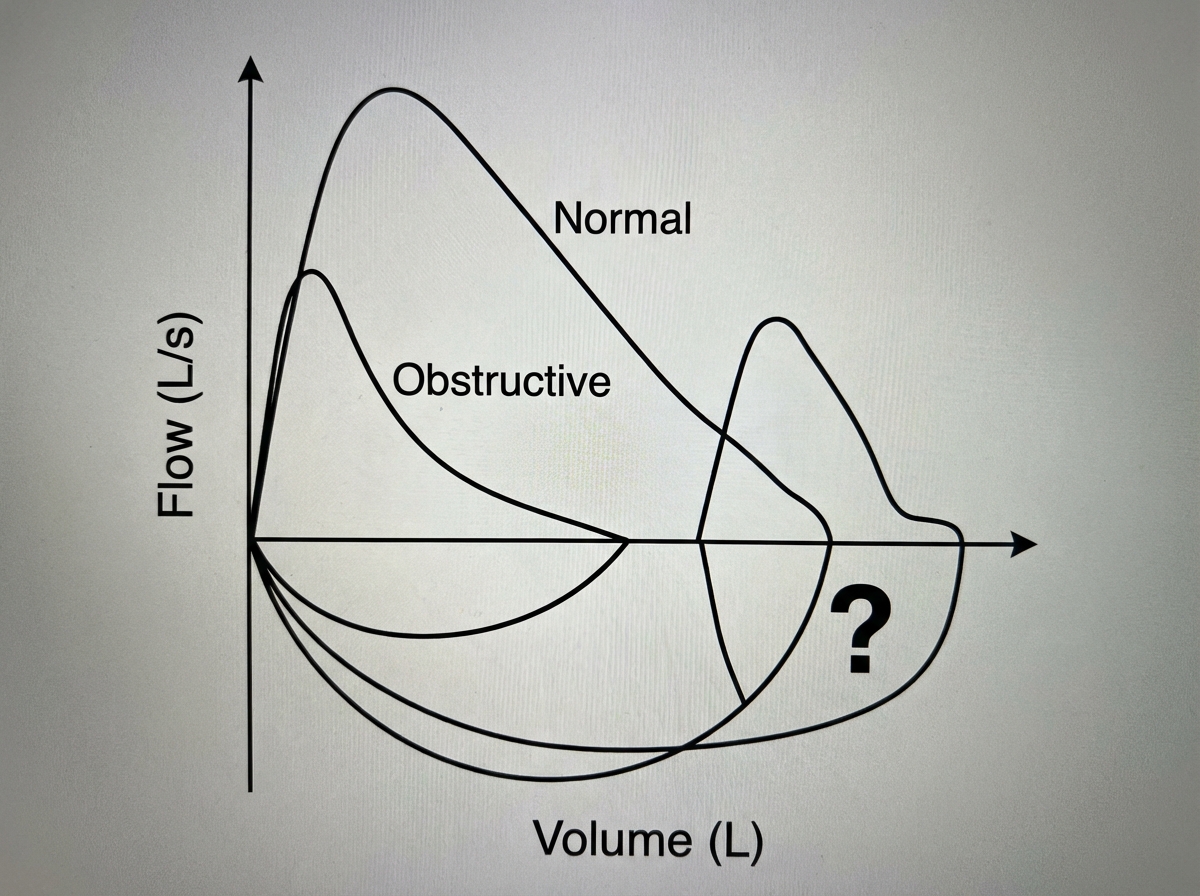
The curve indicated by the question mark is caused by which condition?
What is the volume of air in the lungs after a normal expiration called?
A man has an intrapleural pressure of -5 cm H2O before inspiration and -10 cm H2O at the end of inspiration. He inspires 1200 ml. What is the compliance of the lungs?
Kussmaul respiration occurs in response to what condition?
What is an important non-respiratory function of the lungs?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app