
Respiratory System — MCQs

On this page
All of the following are risks seen in the administration of pure oxygen to hypoxic patients, except?
What is the major role of 2,3-DPG in red blood cells?
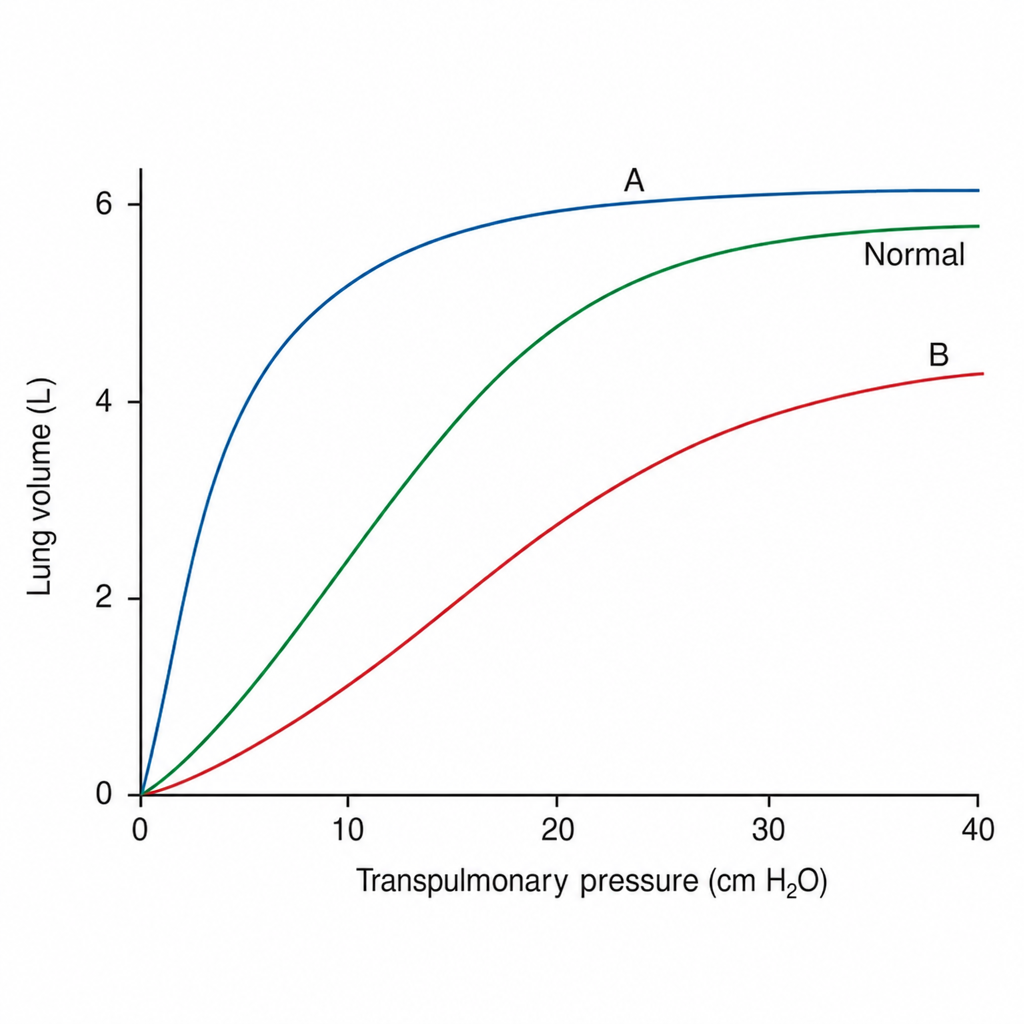
The compliance curve of the lung is shown below. Curve A signifies which of the following?
In the work of breathing, what percentage fraction does tissue resistance contribute?
What is the normal partial pressure of oxygen (PaO2) in a healthy adult?
What is the sensitivity of chemoreceptors in COPD?
Vital capacity is the sum of which of the following?
Compared to the base, the apex of the upright human lung has:
Hypoxic pulmonary vasoconstriction:
Which of the following conditions is NOT associated with a decrease in Residual Volume?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app