
Respiratory System — MCQs

On this page
Peripheral chemoreceptors are maximally stimulated by which of the following?
Compliance of the lung is measured by?
What is the normal ratio of forced expiratory volume in the first second (FEV1) to the forced vital capacity (FVC) in an adult male?
Which gas is used to measure the diffusing capacity of the lungs?
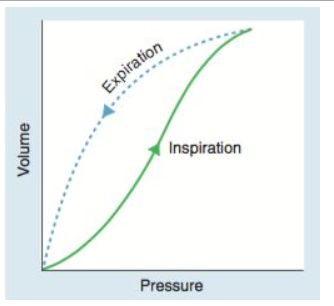
The provided graph illustrates the relationship between lung volume and transpulmonary pressure in a static lung pressure-volume curve during inspiration and expiration. What is the most likely explanation for the observed pattern?
What is the effect of cutting the spinal cord above the medulla on respiration?
Laminar flow is dependent on which of the following factors?
Binding of O2 to hemoglobin reduces its affinity for CO2 by which effect?
Which of the following is seen in pneumothorax?
During inspiration, what is the main pathway of airflow in a normal nasal cavity?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app