
Respiratory System — MCQs

On this page
What causes the chloride shift?
Among which types of hypoxia is the arteriovenous oxygen difference maximized?
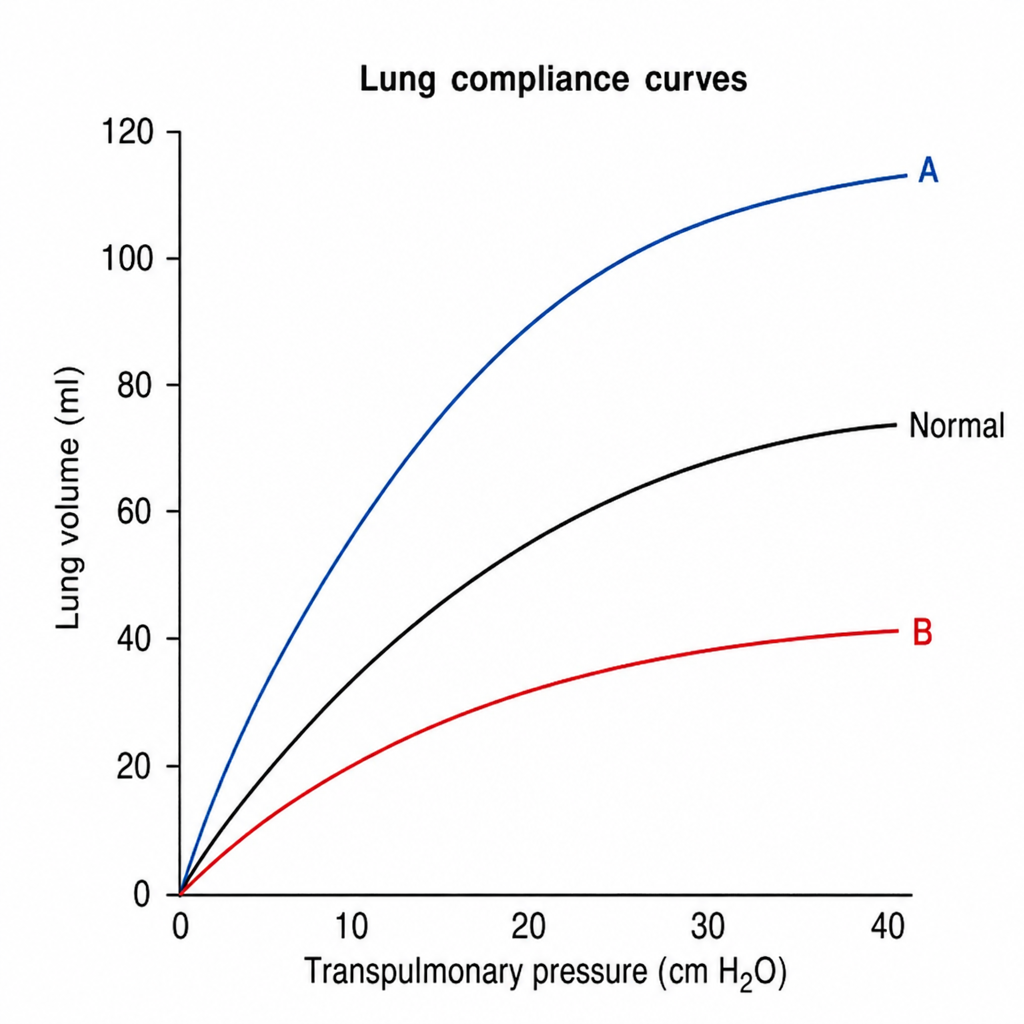
What does Curve A signify in the given lung compliance curve?
At the end of normal expiration, what is the state of the respiratory system?
A subject inhales a mixture of gases containing carbon monoxide and holds his breath for 10 seconds. During this period, the alveolar PCO is 0.5 mmHg and the CO uptake is 25 ml/min. Which of the following is the diffusing capacity of the lung for CO?
What is the approximate level of oxygen in the blood when 100% oxygen is administered under atmospheric pressure?
During normal quiet breathing, in which of the following is the maximum work done?
What is the primary function of the mucociliary action in the upper respiratory tract?
Which of the following conditions does not usually cause a reduction in Diffusion Lung Capacity for Carbon Monoxide (DLCO)?
Oxyhemoglobin saturation does not depend upon which of the following factors?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app