
Respiratory System — MCQs

On this page
What is Critical Closing Volume?
Which of the following has the highest affinity for hemoglobin?
A transaction at the mid-pons level with intact vagi leads to which type of breathing pattern?
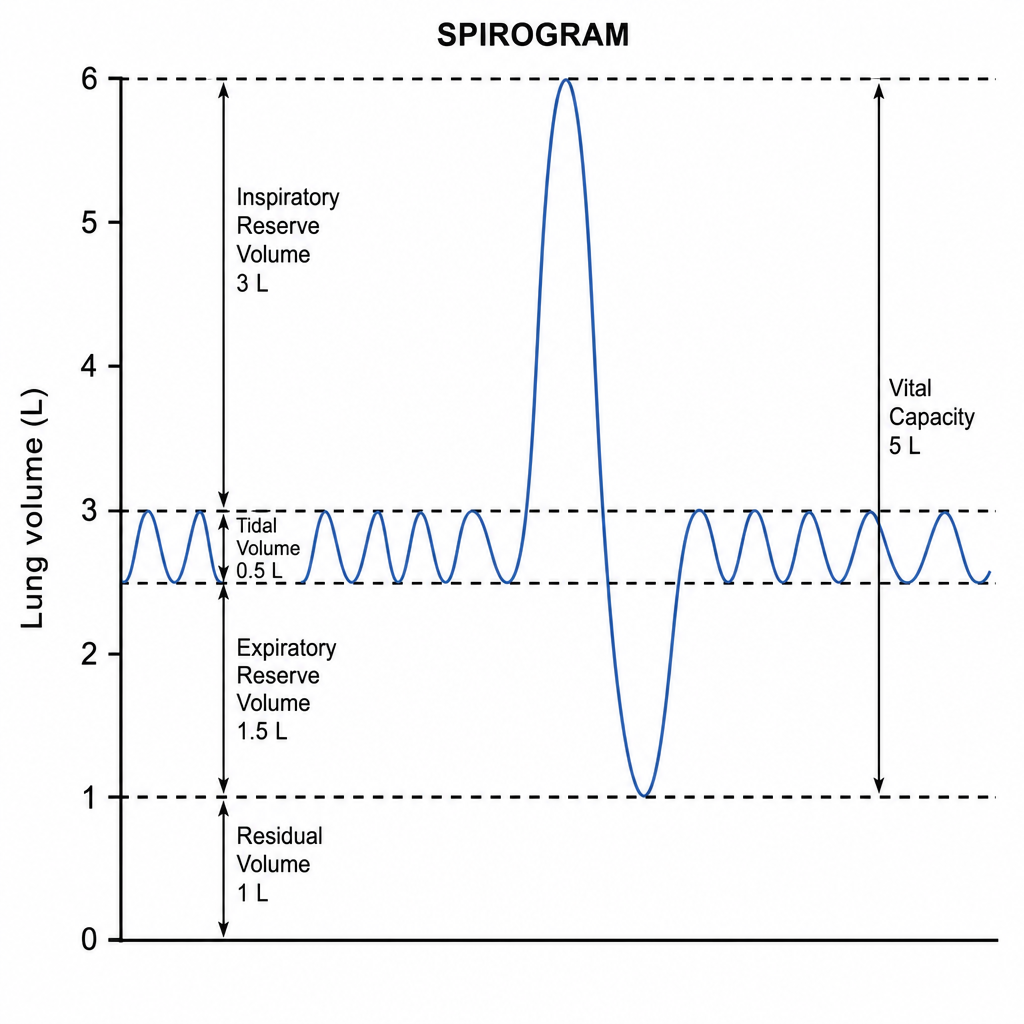
Calculate the minute ventilation from the spirogram assuming the respiratory rate as 12/min?
The ratio of carbon dioxide produced to oxygen consumed is known as what?
Which of the following variants of hypoxia does not stimulate peripheral chemoreceptors?
What is the percentage of normal physiological dead space?
Which of the following statements concerning airflow in the lung is TRUE?
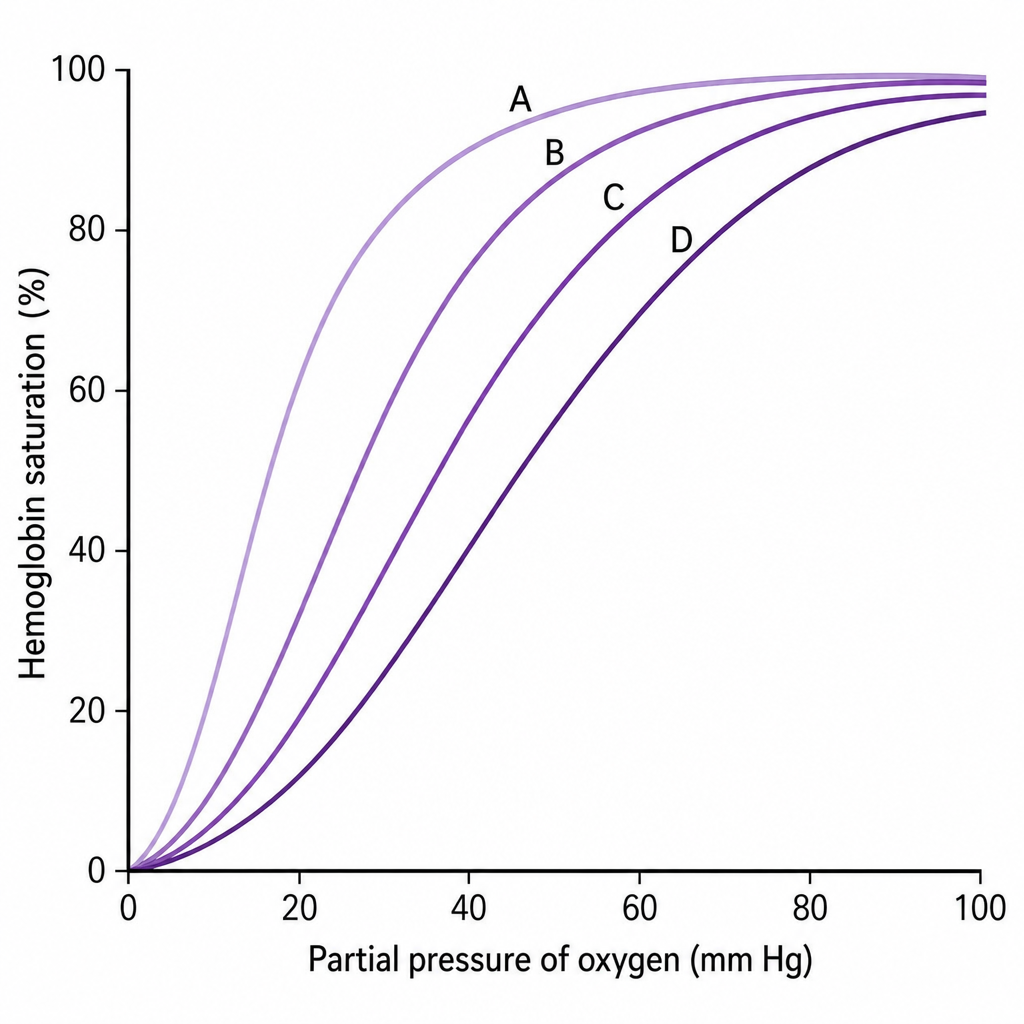
Which of the following oxygen-hemoglobin dissociation curves corresponds to blood during resting (dark purple line) and during exercise (light purple line)?
What is the normal tidal volume in a resting man?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app