
Respiratory System — MCQs

On this page
What is the anatomical dead space of a normal lung?
In a normal resting person breathing air at sea level, what is the alveolar partial pressure of oxygen (in mm Hg)?
The pneumotaxic center is located in which part of the brain?
Which physiological parameter is almost the same at the apex and base of the lung?
The physiological dead space is decreased by:
The slope of the pressure-volume curve of the lung represents which of the following?
A 5-year-old child at sea level has the following arterial blood gas results: pH 7.41, PaO2 100 mmHg, and PaCO2 40 mmHg. The child is being ventilated with 80% oxygen. What is the alveolar-arterial oxygen gradient (A-a PO2)?
The condition in which the arterial PO2 is normal but the amount of hemoglobin available to carry O2 is reduced?
Which of the following statements is true regarding the Hb/O2 dissociation curve?
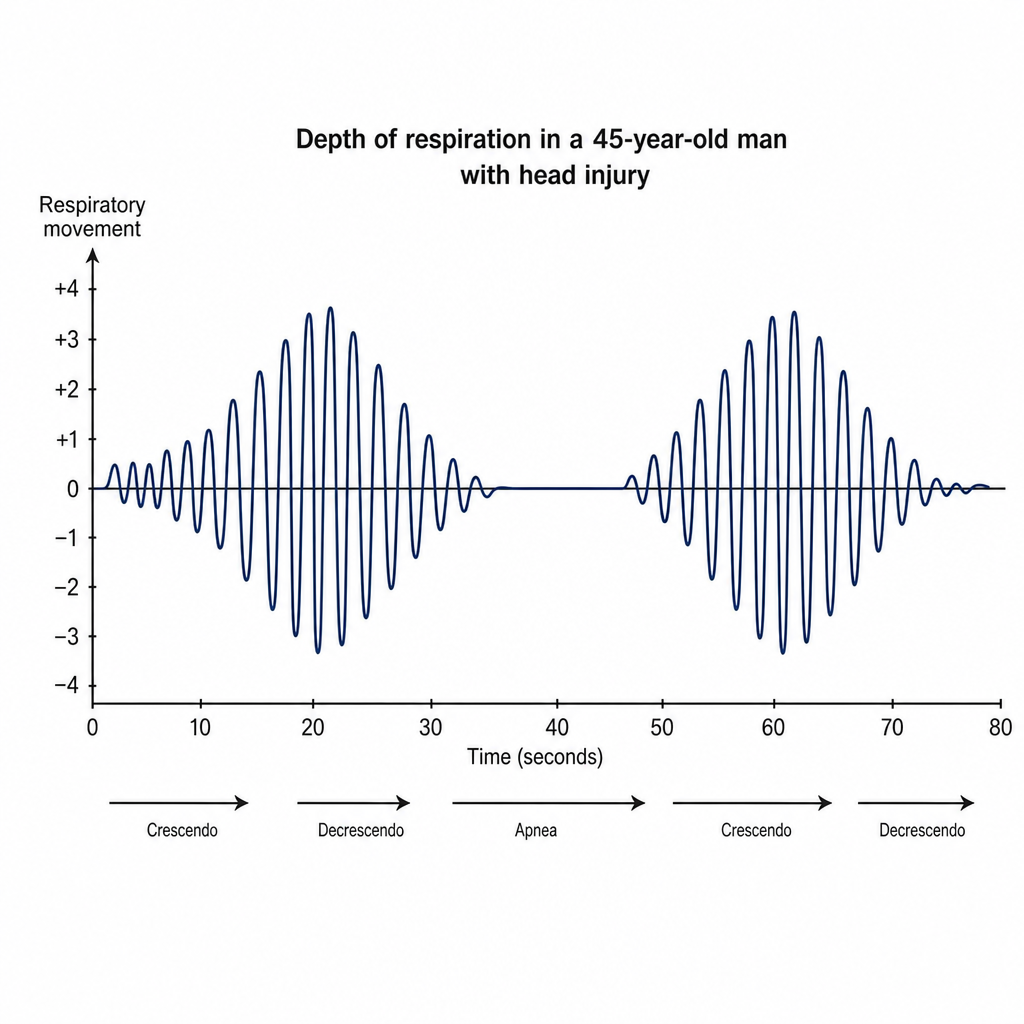
The provided diagram shows the depth of respiration of a 45-year-old man who suffered a head injury in an automobile accident. This crescendo-decrescendo pattern of breathing is known as:
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app