
Diving Physiology — MCQs

What is the physiological response of the kidney during shock?
What type of narcosis is primarily associated with increased nitrogen solubility under pressure?
A 69-year-old man has an abnormally increased curvature of the thoracic vertebral column. Which of the following conditions is the most likely diagnosis?
Regarding Caisson's disease which statement among the following is CORRECT?
What is the estimated PaO2 after giving FiO2 at 0.5 in a normal person?
Which equation is used to calculate physiological dead space?
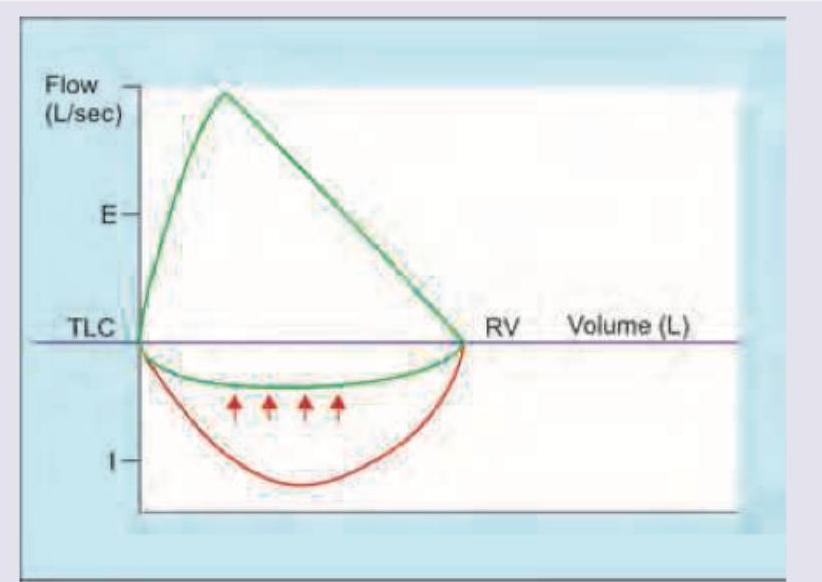
Which flow volume curve recording is shown below?
Cushing reflex is associated with all except?
Nociceptive signals from the face and head are transmitted primarily to which of the following?
Complete transection of the spinal cord at the C7 level produces all of the following effects except:
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app