
Respiratory System — MCQs

On this page
A patient undergoes a surgery where one lung is removed due to malignancy. Which of the following parameters should be measured to accurately assess the remaining lung's elasticity, independent of the change in lung volume?
Identify the breathing pattern shown in the image below:
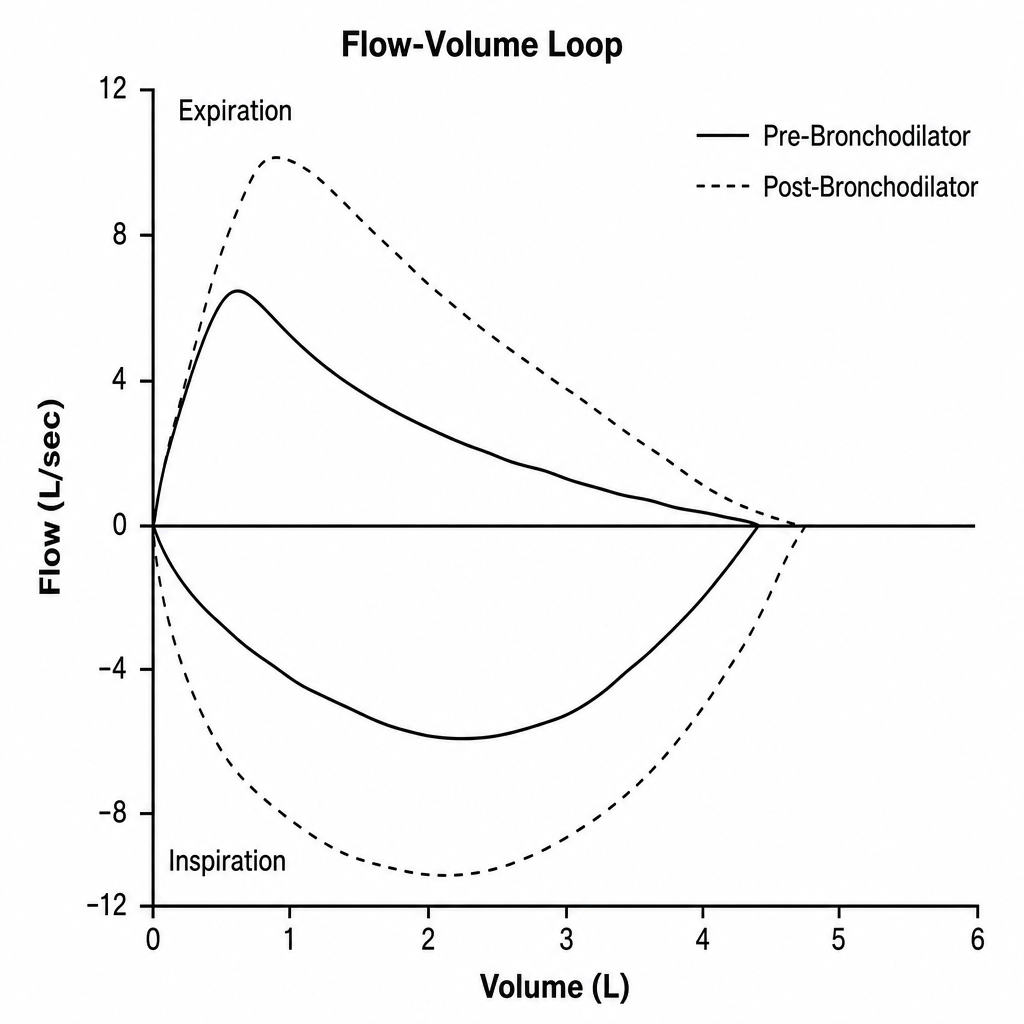
A 58-year-old male with a 35 pack-year smoking history presents with progressive exertional dyspnoea and a chronic productive cough for the past 4 years. Spirometry is performed before and after bronchodilator administration. The tracing obtained is shown (Image 1). Which of the following best explains the characteristic shape of the expiratory limb seen in this tracing?
A 68-year-old man with both severe COPD (emphysema) and newly diagnosed idiopathic pulmonary fibrosis presents with worsening dyspnea. His pressure-volume curve shows a complex pattern with features of both diseases. Static compliance measured at mid-lung volumes is 120 mL/cm H2O. His pulmonologist must decide on optimal management. Synthesizing the pathophysiology of both conditions, what represents the most significant clinical challenge in managing his combined disease?
A 42-year-old woman with systemic sclerosis develops both pulmonary fibrosis and chest wall restriction from skin thickening. Her measured total respiratory system compliance is 30 mL/cm H2O. Testing with complete paralysis and positive pressure ventilation shows isolated lung compliance of 50 mL/cm H2O. She is being considered for immunosuppressive therapy versus supportive care. Evaluate which intervention would provide the greatest improvement in her respiratory mechanics.
A 58-year-old man with end-stage pulmonary fibrosis is being evaluated for lung transplantation. His current static compliance is 25 mL/cm H2O (normal: 200 mL/cm H2O). He also has mild obesity (BMI 32) and ankylosing spondylitis affecting chest wall mobility. Post-transplant, assuming successful bilateral lung transplant with normal donor lungs, what would be the expected change in his total respiratory system compliance?
A research study compares two patients with different lung pathologies but identical functional residual capacity (FRC) of 3.0 L. Patient A has pulmonary fibrosis with FRC above the steep portion of the compliance curve. Patient B has emphysema with FRC on the flat upper portion of the curve. Both attempt to inhale the same tidal volume. Analyzing their work of breathing, which statement best characterizes the difference?
A 32-year-old woman develops acute respiratory distress syndrome (ARDS) following sepsis. She is mechanically ventilated with tidal volume 450 mL and plateau pressure 35 cm H2O (PEEP 10 cm H2O). Her static compliance is calculated as 18 mL/cm H2O. The team considers changing ventilator settings. Analyzing her respiratory mechanics, what change would most effectively improve compliance while minimizing ventilator-induced lung injury?
A 55-year-old woman with idiopathic pulmonary fibrosis and a 40-year-old man with severe emphysema both have the same total lung capacity of 4.5 L on pulmonary function testing. However, their pressure-volume curves show opposite patterns. During inspiration from FRC, which patient requires greater change in pleural pressure to achieve the same tidal volume, and why?
A 70-year-old man with severe kyphoscoliosis presents with chronic dyspnea. Pulmonary function testing shows reduced total lung capacity and functional residual capacity. His lung tissue biopsy is normal, but respiratory muscle strength testing shows normal values. Analysis of his pressure-volume curve shows a normal curve for lung tissue alone, but decreased total respiratory system compliance. What explains his respiratory mechanics?
Practice by Chapter
Mechanics of Breathing
Practice Questions
Pulmonary Ventilation
Practice Questions
Pulmonary Circulation
Practice Questions
Gas Exchange in the Lungs
Practice Questions
Oxygen and Carbon Dioxide Transport
Practice Questions
Control of Breathing
Practice Questions
Respiratory Adjustments in Health and Disease
Practice Questions
High Altitude Physiology
Practice Questions
Diving Physiology
Practice Questions
Respiratory Function Tests
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app