
Reproductive Physiology — MCQs

On this page
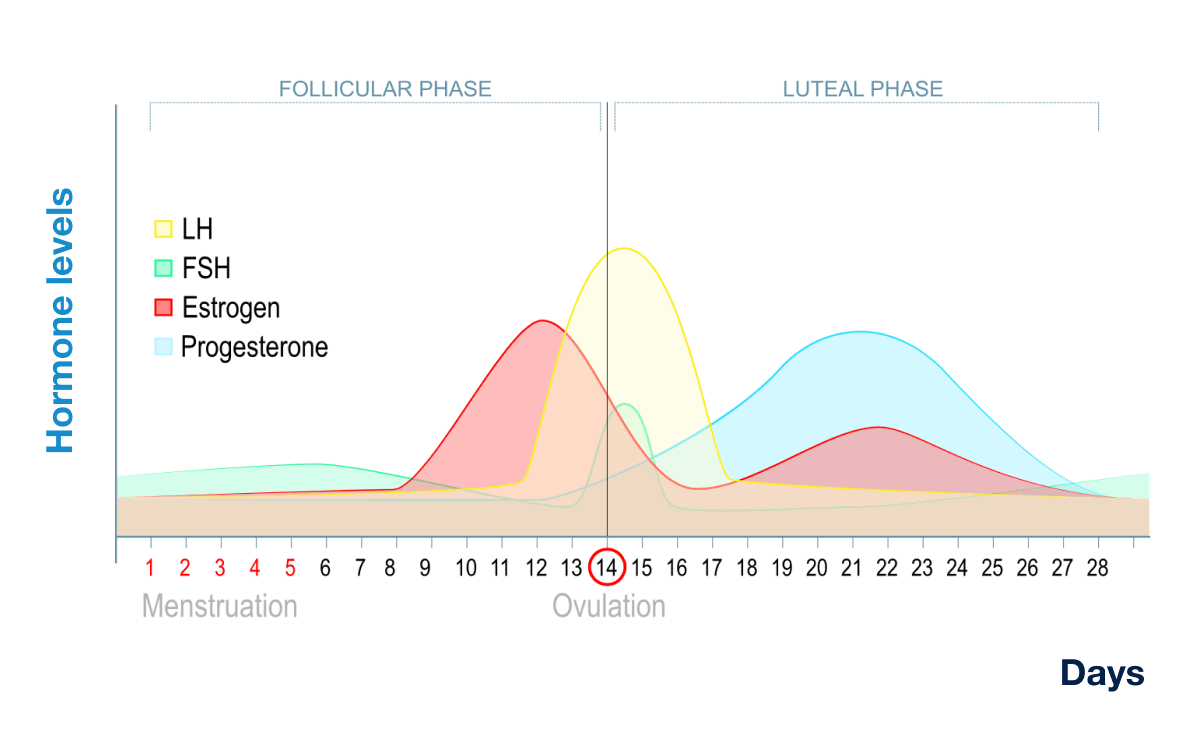
At the time point indicated by the arrow, the hormone levels relative to their early-follicular phase baseline are:
Testis is not the source for which of the following?
Sertoli cells secrete ?
A major function of the epididymis is:
Spermatogenesis occurs at which temperature condition?
Which of the following is not secreted by Sertoli cells?
Order of development of secondary sexual characteristic in male –
Levels of which of the following hormones are increased in postmenopausal women:
Sertoli cells play a key role in which of the following processes?
Which hormone binds to the receptors on Leydig cells?
Practice by Chapter
Male Reproductive Physiology
Practice Questions
Spermatogenesis and Sperm Function
Practice Questions
Female Reproductive Physiology
Practice Questions
Menstrual Cycle
Practice Questions
Ovulation and Fertilization
Practice Questions
Physiology of Pregnancy
Practice Questions
Parturition
Practice Questions
Lactation
Practice Questions
Sexual Differentiation and Development
Practice Questions
Reproductive Aging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app