
Reproductive Physiology — MCQs

On this page
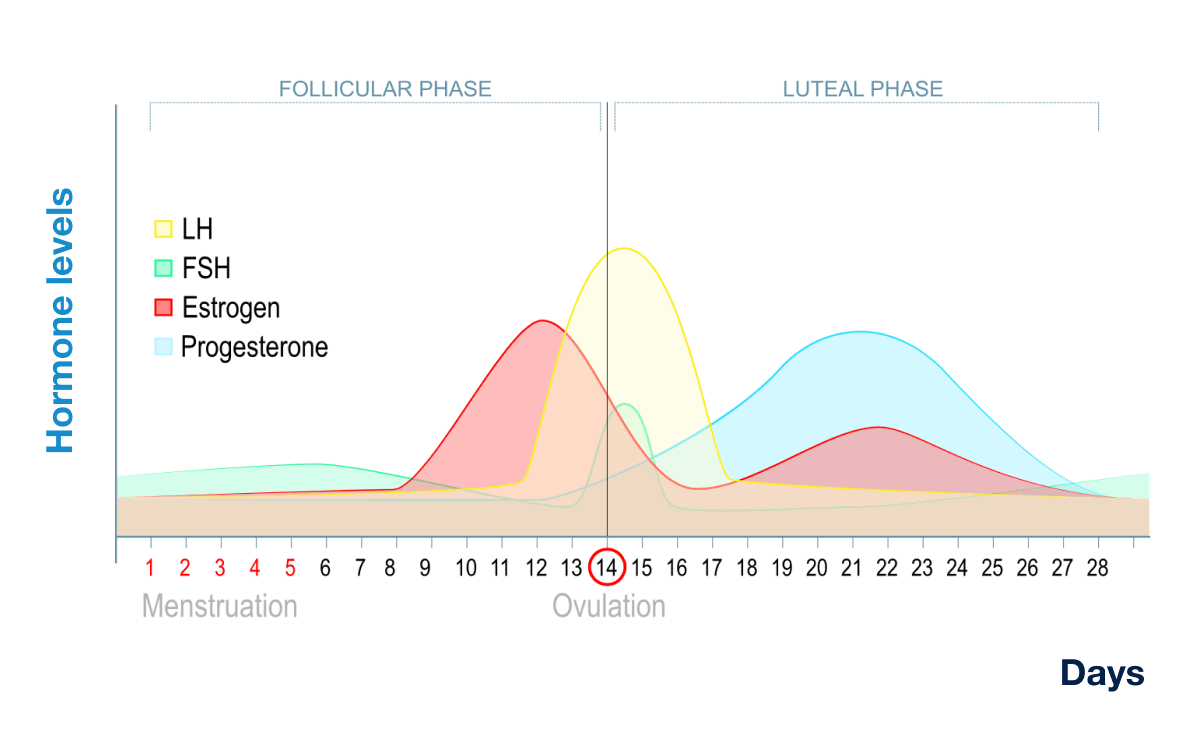
In this normal menstrual cycle graph, the mark 'X' represents levels of which hormone?
Testosterone is secreted by:
Inhibin is secreted by:
There is a mid-cycle shift in the basal body temperature (BBT) after ovulation in women. This is caused by :
Dihydrotestosterone acts on
Transplacental exchanges that take place are essential to the well being of the fetus. Which of those listed below is NOT a method?
Ovulation is primarily caused by preovulatory surge of:
Which hormones antagonize the effect of NO and cause the penis to become flaccid after orgasm?
Progesterone production in the ovary is primarily by:
Spermatogenesis is mostly controlled by:
Practice by Chapter
Male Reproductive Physiology
Practice Questions
Spermatogenesis and Sperm Function
Practice Questions
Female Reproductive Physiology
Practice Questions
Menstrual Cycle
Practice Questions
Ovulation and Fertilization
Practice Questions
Physiology of Pregnancy
Practice Questions
Parturition
Practice Questions
Lactation
Practice Questions
Sexual Differentiation and Development
Practice Questions
Reproductive Aging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app