
Reproductive Physiology — MCQs

On this page
The placenta secretes a hormone that is utilized in the early detection of pregnancy. This hormone is:
Which among the following hormones acts on post ovulatory endometrium?
Which among the following hormones, in a lactating mother, is responsible for the maintenance and proliferation of milk-secreting breast tissue?
Hormone responsible for milk ejection reflex in the image shown?
During spermatogenesis, which of the following hormones inhibits Follicle-Stimulating Hormone (FSH) secretion?
What is the cause of LH (Luteinizing Hormone) surge?
In a woman with a regular 28-day menstrual cycle, which of the following best describes the typical hormonal profile during days 21 to 25 of the cycle?
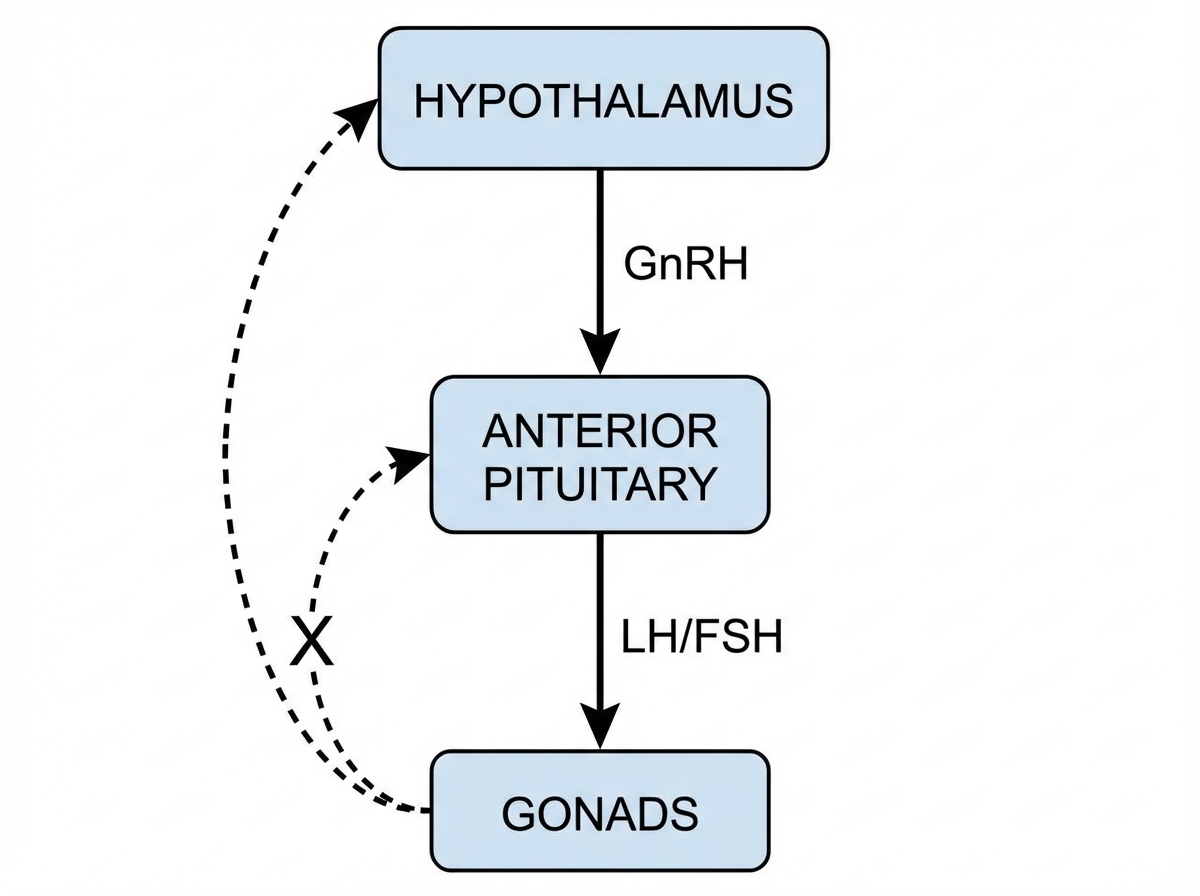
Which hormones provide the general sex-steroid feedback represented by $X$ in both male and female HPG axes?
Carbohydrate metabolism in normal pregnancy shows :
Onset of labour is initiated by which of the following?
Practice by Chapter
Male Reproductive Physiology
Practice Questions
Spermatogenesis and Sperm Function
Practice Questions
Female Reproductive Physiology
Practice Questions
Menstrual Cycle
Practice Questions
Ovulation and Fertilization
Practice Questions
Physiology of Pregnancy
Practice Questions
Parturition
Practice Questions
Lactation
Practice Questions
Sexual Differentiation and Development
Practice Questions
Reproductive Aging
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app