
Renal Physiology — MCQs

On this page
In which region of the nephron are P cells (principal cells) located?
What is the exact number of solutes transported in the thick ascending limb of the Loop of Henle per carrier pump?
Which of the following statements is true regarding calcium reabsorption in the kidney?
Glucose is absorbed through the apical membrane of the proximal convoluted tubule by which transporter?
Free water clearance by the kidney is increased by which of the following?
In a cystometrogram, where does LaPlace's law have its primary application?
A 20-year-old male patient presents with a decrease in urinary output to about 400ml/day. Both renal blood flow (RBF) and glomerular filtration rate (GFR) were decreased. Which of the following causes a decrease in both RBF and GFR?
Which of the following can reduce the glomerular filtration rate (GFR)?
A 78-year-old man presents with nausea and vomiting. On examination, he appears dehydrated, his abdomen is soft, and the jugular venous pressure is not elevated. Laboratory tests reveal hypernatremia, and his calculated free water deficit is approximately 3 L. In which part of the normal kidney is most of the water reabsorbed?
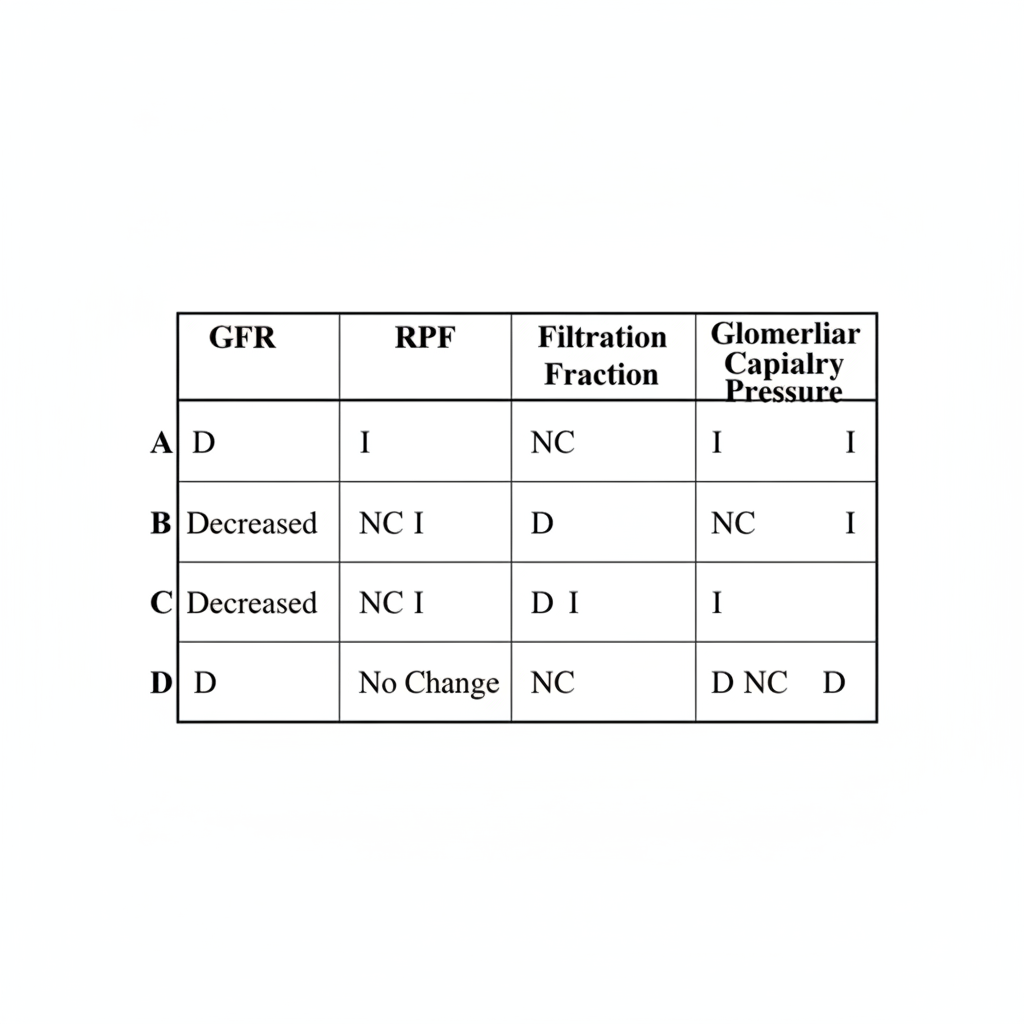
A patient is given a drug that dilates the afferent arteriole and contracts the efferent arteriole, leaving total renal vascular resistance unchanged. Which set of changes is likely to occur in the following table? (I = increased, D = decreased, NC = no change)
Practice by Chapter
Renal Blood Flow and Glomerular Filtration
Practice Questions
Tubular Reabsorption and Secretion
Practice Questions
Concentration and Dilution of Urine
Practice Questions
Acid-Base Regulation by the Kidneys
Practice Questions
Sodium and Water Balance
Practice Questions
Potassium Regulation
Practice Questions
Calcium and Phosphate Handling
Practice Questions
Micturition Physiology
Practice Questions
Renal Function Tests
Practice Questions
Integrative Responses to Fluid Challenges
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app