
Renal Physiology — MCQs

On this page
Which of the following statements is true regarding the function of the distal convoluted tubule?
Which of the following statements about aquaporins is false?
Plasma inulin of a person is 4 mg/ml and urine flow rate is 20 ml/min. What will be GFR if urine inulin is 50 mg/ml?
What decreases renin secretion?
What is the primary function of Lacis cells in the nephron?
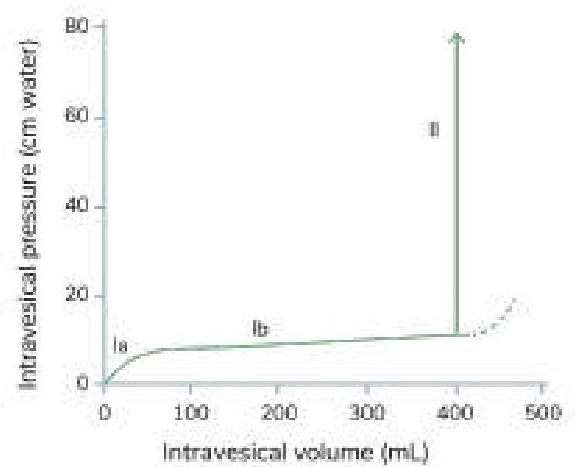
Which of the following statements is true regarding the given cystometrogram?
Impaired function of Aquaporin results in
Which of the following is NOT a component responsible for the counter current mechanism in the kidney?
Vasopressin acts through which aquaporin channels in the collecting duct?
What is the physiological response of the kidney during shock?
Practice by Chapter
Renal Blood Flow and Glomerular Filtration
Practice Questions
Tubular Reabsorption and Secretion
Practice Questions
Concentration and Dilution of Urine
Practice Questions
Acid-Base Regulation by the Kidneys
Practice Questions
Sodium and Water Balance
Practice Questions
Potassium Regulation
Practice Questions
Calcium and Phosphate Handling
Practice Questions
Micturition Physiology
Practice Questions
Renal Function Tests
Practice Questions
Integrative Responses to Fluid Challenges
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app