
Neurophysiology — MCQs

On this page
Which of the following statements about cerebellar neuronal connections is correct?
Which of the following is referred to as the "Window of the limbic system"?
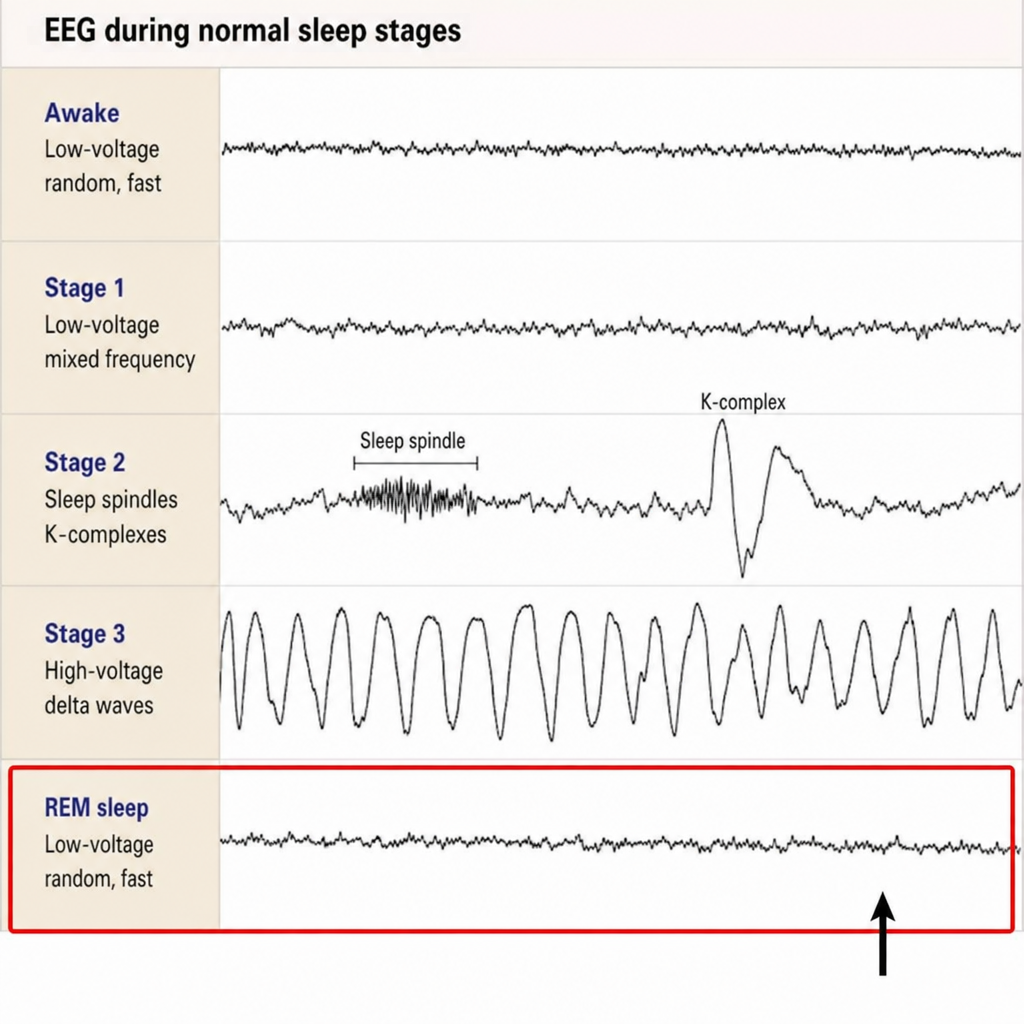
A polysomnogram epoch shows an unlabeled EEG channel with low-amplitude, mixed-frequency activity, accompanied by rapid eye movements on EOG and muscle atonia on chin EMG. Identify the sleep stage represented by this highlighted tracing.
Type of sensation lost on same side of Brown Sequard syndrome?
Which of the following statements about sleep is incorrect?
Gamma waves of REM sleep are associated with?
Which of the following neurons in the cerebellar cortex is primarily excitatory?
Which part of the sympathetic nervous system is responsible for secreting catecholamines?
What do motor evoked potentials primarily assess?
What is one of the specific functions of the primary motor cortex located on the anterior edge of the pre-central gyrus?
Practice by Chapter
Neurons and Glial Cells
Practice Questions
Synaptic Transmission
Practice Questions
Sensory Processing
Practice Questions
Motor Control Systems
Practice Questions
Autonomic Nervous System
Practice Questions
Hypothalamus and Limbic System
Practice Questions
Cerebral Cortex Functions
Practice Questions
Electroencephalography
Practice Questions
Neuroplasticity
Practice Questions
Sleep and Wakefulness
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app