
Neurophysiology — MCQs

On this page
EEG waves prominent in occipital lobe are
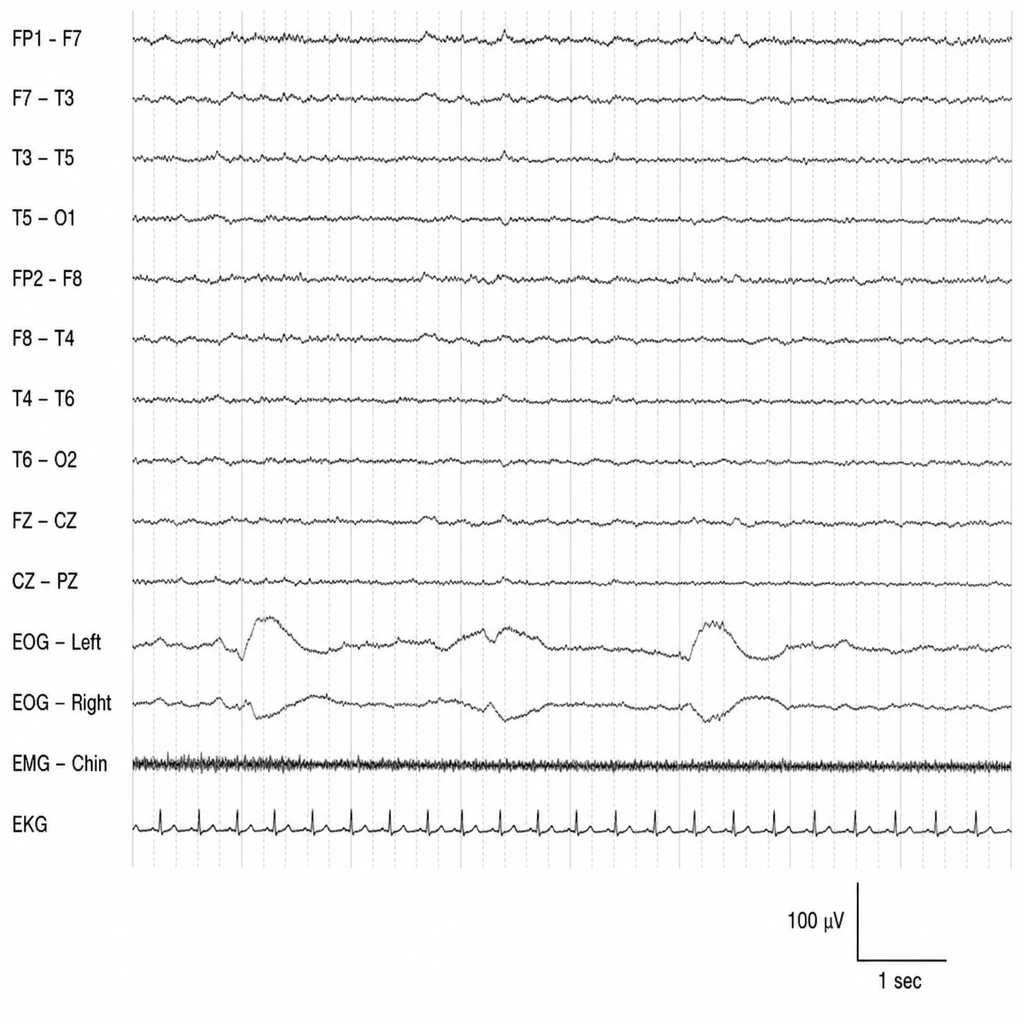
The EEG recorded shown below is normally recordable during which stage of sleep?
All of the following are known functions of hypothalamus except
Ablation of the somatosensory area I of the cerebral cortex leads to
Which of the following acts as the major neurotransmitter in the substantia nigra?
True statement about cerebrospinal fluid is
The rigidity seen in Parkinson's disease is due to
Mechanical stimulation of the pain-sensitive structures of the brain can cause headache. All of the following are pain-sensitive structures of the brain, EXCEPT?
A patient came to OPD with a stamping gait. On examination,when he was asked to close his eyes and walk, he fails to walk. Which of the following tracts is most probably affected?
The EEG pattern in REM sleep is:
Practice by Chapter
Neurons and Glial Cells
Practice Questions
Synaptic Transmission
Practice Questions
Sensory Processing
Practice Questions
Motor Control Systems
Practice Questions
Autonomic Nervous System
Practice Questions
Hypothalamus and Limbic System
Practice Questions
Cerebral Cortex Functions
Practice Questions
Electroencephalography
Practice Questions
Neuroplasticity
Practice Questions
Sleep and Wakefulness
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app