
Neurophysiology — MCQs

On this page
A patient is experiencing phantom limb pain after the amputation of the right limb. What is observed on a PET scan in a patient with phantom limb pain?
What are the effects of a lesion in Brodmann area 22?
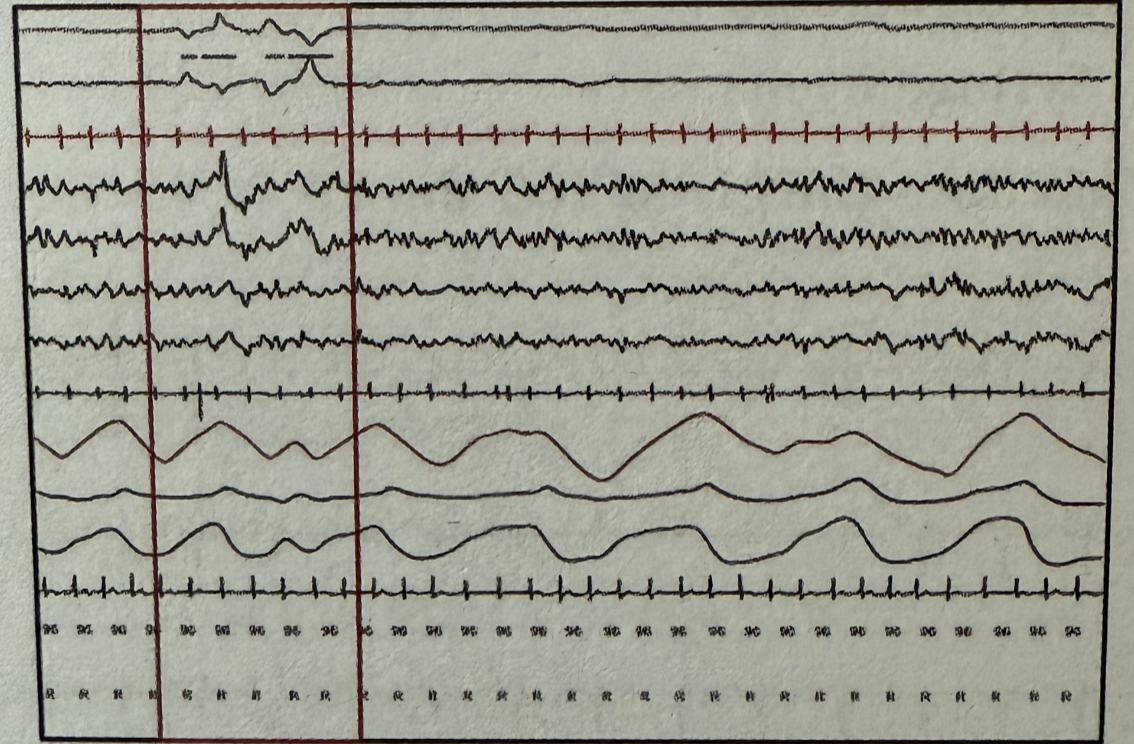
During polysomnography, which stage of sleep is represented by the marked areas when observing the following wave patterns? EOG (Electrooculography) EEG (Electroencephalography) EMG (Electromyography)
A woman with right-sided loss of sensations of both the upper and lower limb complains of shooting pain from her fingers to the right shoulder and a burning sensation when touching cold water. Motor functions are normal. Which of the following structures is likely to be involved?
Which change in CSF production most directly affects intracranial pressure?
Which receptor type mediates the slow phase of synaptic transmission in autonomic ganglia?
Which muscle tendon is stretched in patellar tendon reflex?
The primary dopaminergic reward center in the brain is?
Which of the following has small representation in somatosensory area of cerebral cortex -
Which of the following is not carried in dorsal column of spinal cord:
Practice by Chapter
Neurons and Glial Cells
Practice Questions
Synaptic Transmission
Practice Questions
Sensory Processing
Practice Questions
Motor Control Systems
Practice Questions
Autonomic Nervous System
Practice Questions
Hypothalamus and Limbic System
Practice Questions
Cerebral Cortex Functions
Practice Questions
Electroencephalography
Practice Questions
Neuroplasticity
Practice Questions
Sleep and Wakefulness
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app