
Neurophysiology — MCQs

On this page
A lesion in the hippocampus primarily affects which of the following cognitive functions?
In an encephale isolé preparation, transection is done at which level?
All of the following are true regarding the withdrawal reflex except:
What is responsible for the effectiveness of the blood-brain barrier?
Which one of the following indicates the function of the tectospinal tract present in the ventral column of the spinal cord?
What is the approximate daily rate of cerebrospinal fluid (CSF) formation?
On touching the cornea of the right eye, only the right eye blinks. The same response is observed on touching the left eye. Where is the lesion located?
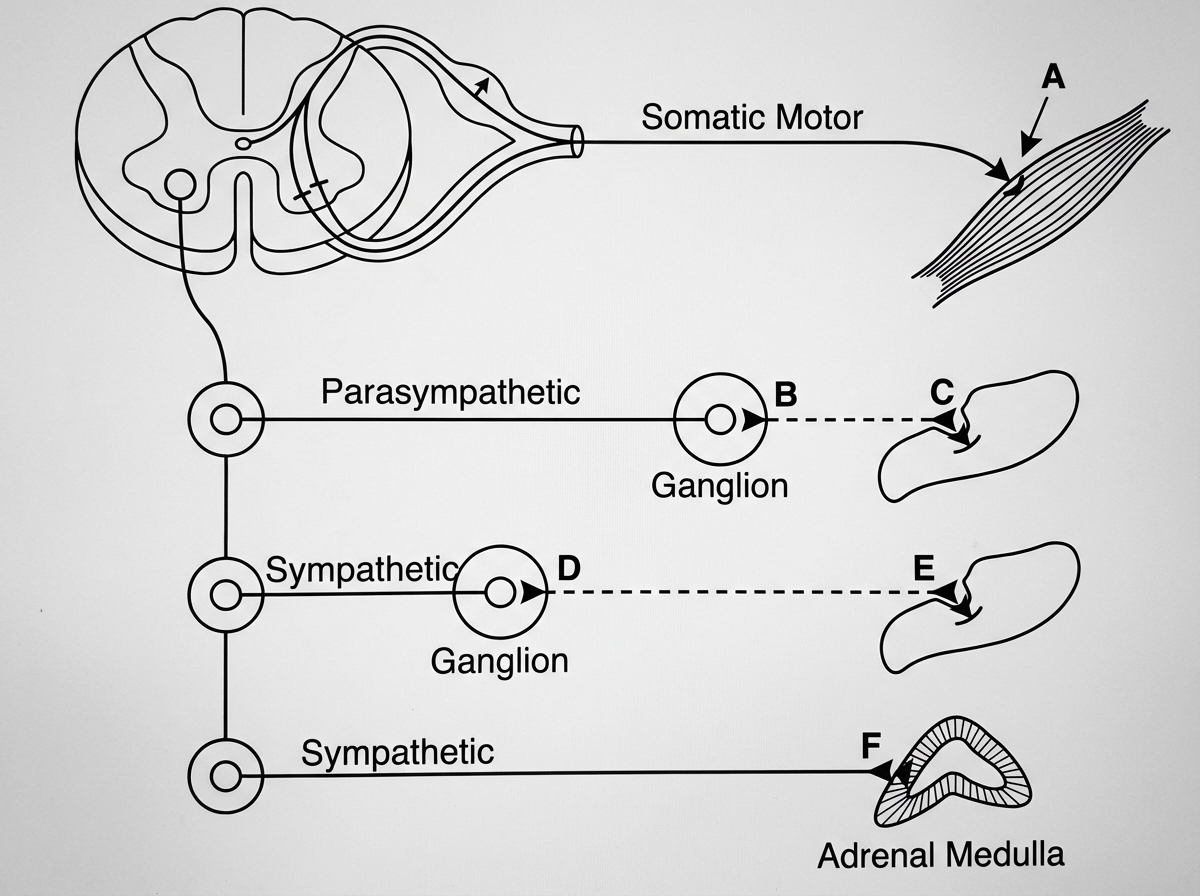
The schematic diagram is depicting some features of the autonomic and somatic nervous systems. What is the neurotransmitter at site 'F'?
K-complex is typically seen in which stage of the sleep cycle?
Damage to which of the following structures is most likely to impair the consolidation of long-term memory?
Practice by Chapter
Neurons and Glial Cells
Practice Questions
Synaptic Transmission
Practice Questions
Sensory Processing
Practice Questions
Motor Control Systems
Practice Questions
Autonomic Nervous System
Practice Questions
Hypothalamus and Limbic System
Practice Questions
Cerebral Cortex Functions
Practice Questions
Electroencephalography
Practice Questions
Neuroplasticity
Practice Questions
Sleep and Wakefulness
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app