
Neurophysiology — MCQs

On this page
Which of the following is not a feature of spinal cord reflex?
Under normal physiological conditions, CSF pressure is proportional to which of the following factors?
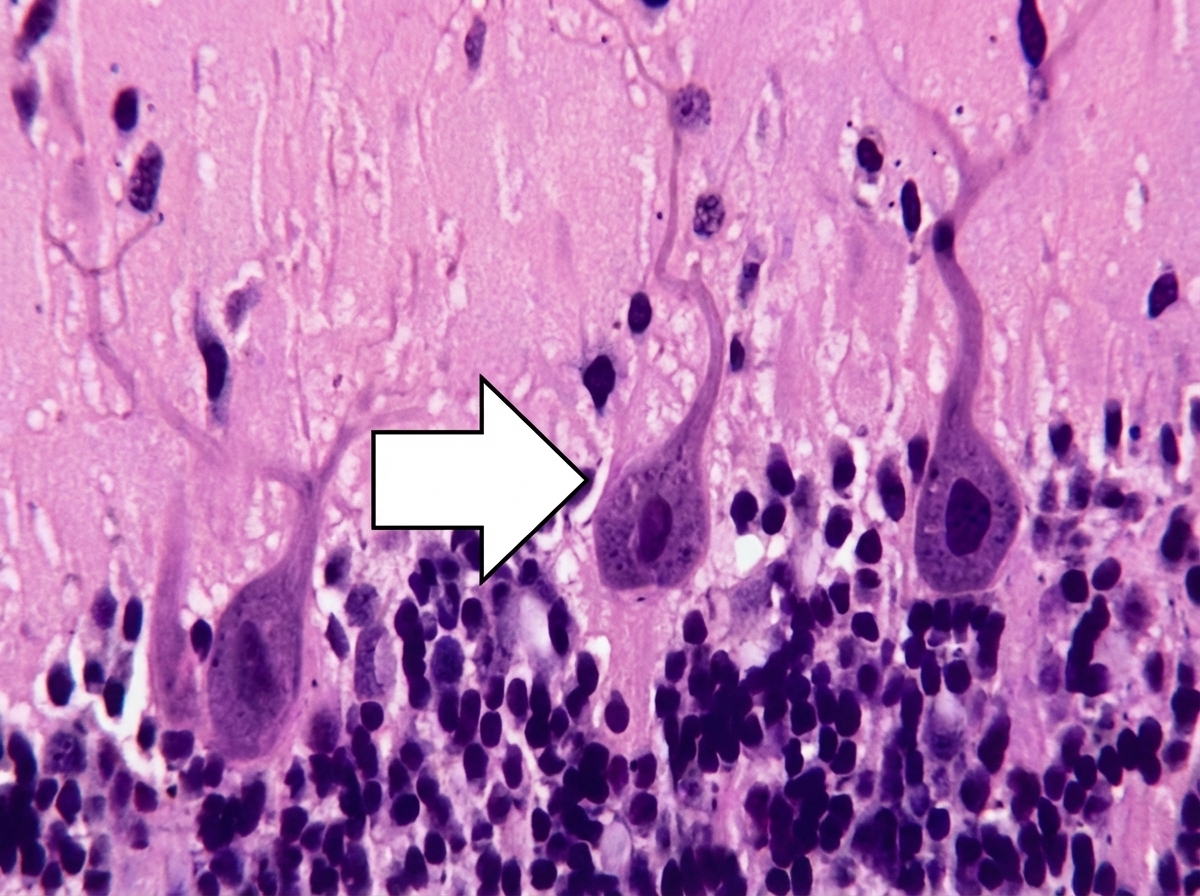
The marked cell (located outside the flocculonodular lobe) inhibits which of the following structure?
What is the sympathetic postganglionic neurotransmitter in sweat glands?
Substance P belongs to the tachykinin family of peptides. Which of the following peripheral tissues contain substance P?
Which afferent fibers are included in the stretch reflex?
Which stage of sleep is characterized by the presence of delta waves on an EEG recording?
Midbrain is the centre for the integration of which of the following reflexes?
Which cranial nerve contributes 75% to the parasympathetic nervous system?
Which of the following is NOT seen in Kluver-Bucy syndrome?
Practice by Chapter
Neurons and Glial Cells
Practice Questions
Synaptic Transmission
Practice Questions
Sensory Processing
Practice Questions
Motor Control Systems
Practice Questions
Autonomic Nervous System
Practice Questions
Hypothalamus and Limbic System
Practice Questions
Cerebral Cortex Functions
Practice Questions
Electroencephalography
Practice Questions
Neuroplasticity
Practice Questions
Sleep and Wakefulness
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app