
Nerve and Muscle Physiology — MCQs

On this page
What is meant by resting muscle length?
Which of the following channelopathies is associated with a calcium channel disorder of muscles?
Which muscle fiber type has a high glycogen content?
Presynaptic facilitation is caused by?
All of the following functions are associated with myelination except?
Which of the following contains the site of attachment for calcium ions that initiates muscle contraction?
Which of the following steps is NOT involved in muscle contraction following a nerve impulse?
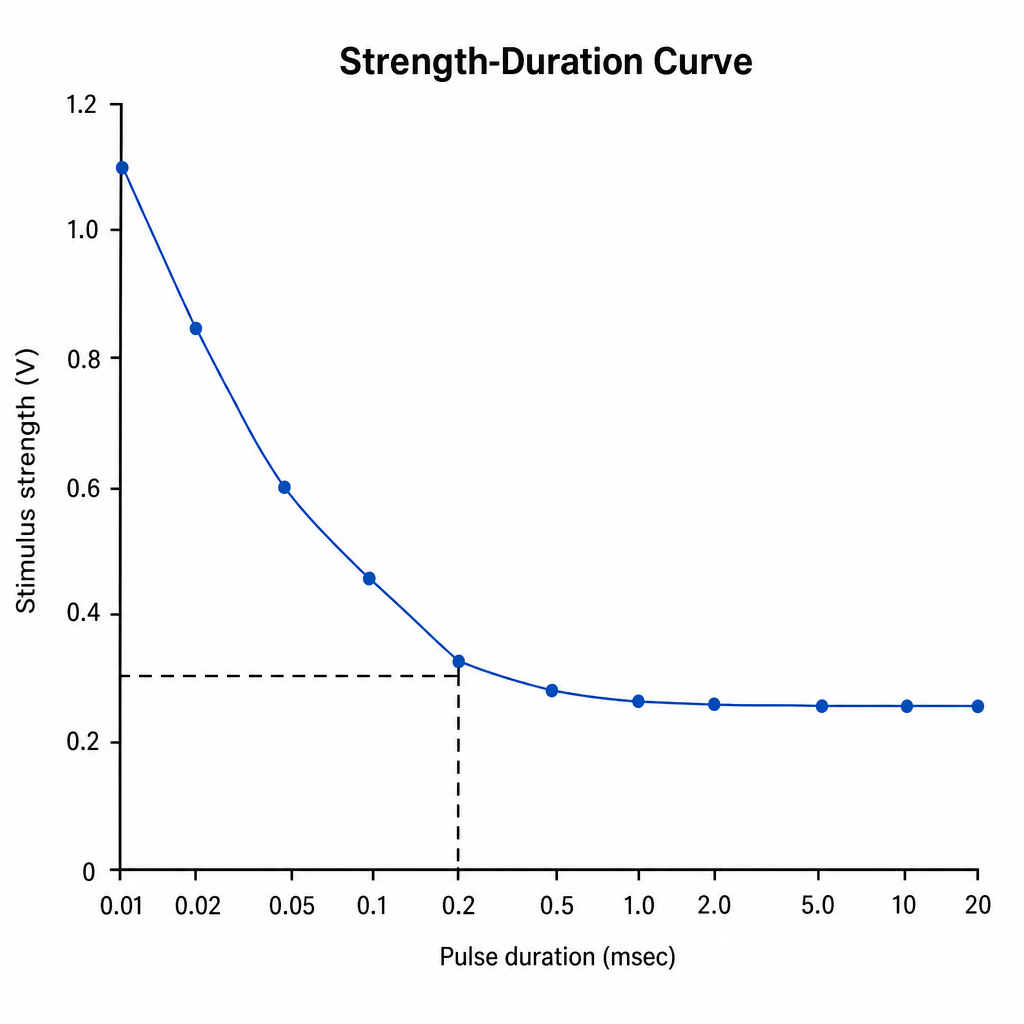
What is the chronaxie minimum?
Rigor mortis results after death is due to which of the following?
Determine the chronaxie and rheobase from the provided graph.
Practice by Chapter
Resting Membrane Potential
Practice Questions
Action Potential Generation and Propagation
Practice Questions
Neuromuscular Junction
Practice Questions
Skeletal Muscle Contraction
Practice Questions
Smooth Muscle Physiology
Practice Questions
Cardiac Muscle Properties
Practice Questions
Muscle Metabolism and Fatigue
Practice Questions
Motor Unit Function
Practice Questions
Neurotransmitters and Receptors
Practice Questions
Electrophysiological Measurements
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app