
Nerve and Muscle Physiology — MCQs

On this page
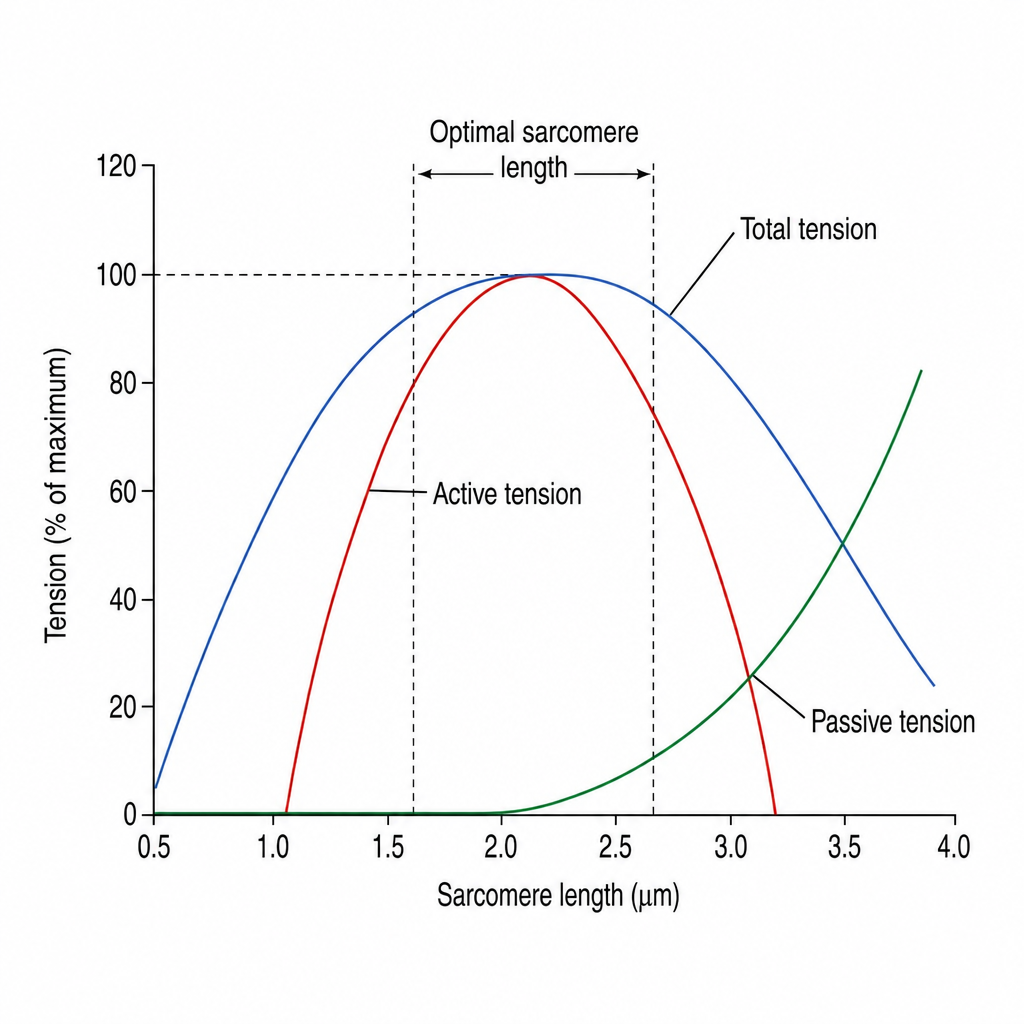
What is the contribution of noncontractile muscle elements to total tension?
Small axons are concerned with all of the following functions, except:
Troponin C mediated function is of which of the following?
Fast pain has a conduction velocity of _____ m/sec?
Increased velocity of conduction in a nerve is caused by:
Which of the following best describes an attribute of visceral smooth muscle that is not shared by skeletal muscle?
Calcium initiates skeletal muscle contraction by which mechanism?
Which muscles are primarily used during the stance and swing phases of normal walking?
Two electrodes are placed 4.5 cm apart. It takes 1.5 ms for current to propagate along the nerve from one electrode to the other. What is the velocity of nerve conduction?
The action of acetylcholine at the neuromuscular junction is terminated primarily by?
Practice by Chapter
Resting Membrane Potential
Practice Questions
Action Potential Generation and Propagation
Practice Questions
Neuromuscular Junction
Practice Questions
Skeletal Muscle Contraction
Practice Questions
Smooth Muscle Physiology
Practice Questions
Cardiac Muscle Properties
Practice Questions
Muscle Metabolism and Fatigue
Practice Questions
Motor Unit Function
Practice Questions
Neurotransmitters and Receptors
Practice Questions
Electrophysiological Measurements
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app