
Nerve and Muscle Physiology — MCQs

On this page
The major source of calcium for contraction of skeletal muscle is:
After-hyperpolarization during nerve conduction is due to:
Which type of muscle exercise involves the muscle changing length against a constant load?
Following traumatic peripheral nerve transection, re-growth usually occurs at which of the following rates?
Which type of motor unit is of prime importance in generating the muscle power necessary for the maintenance of posture?
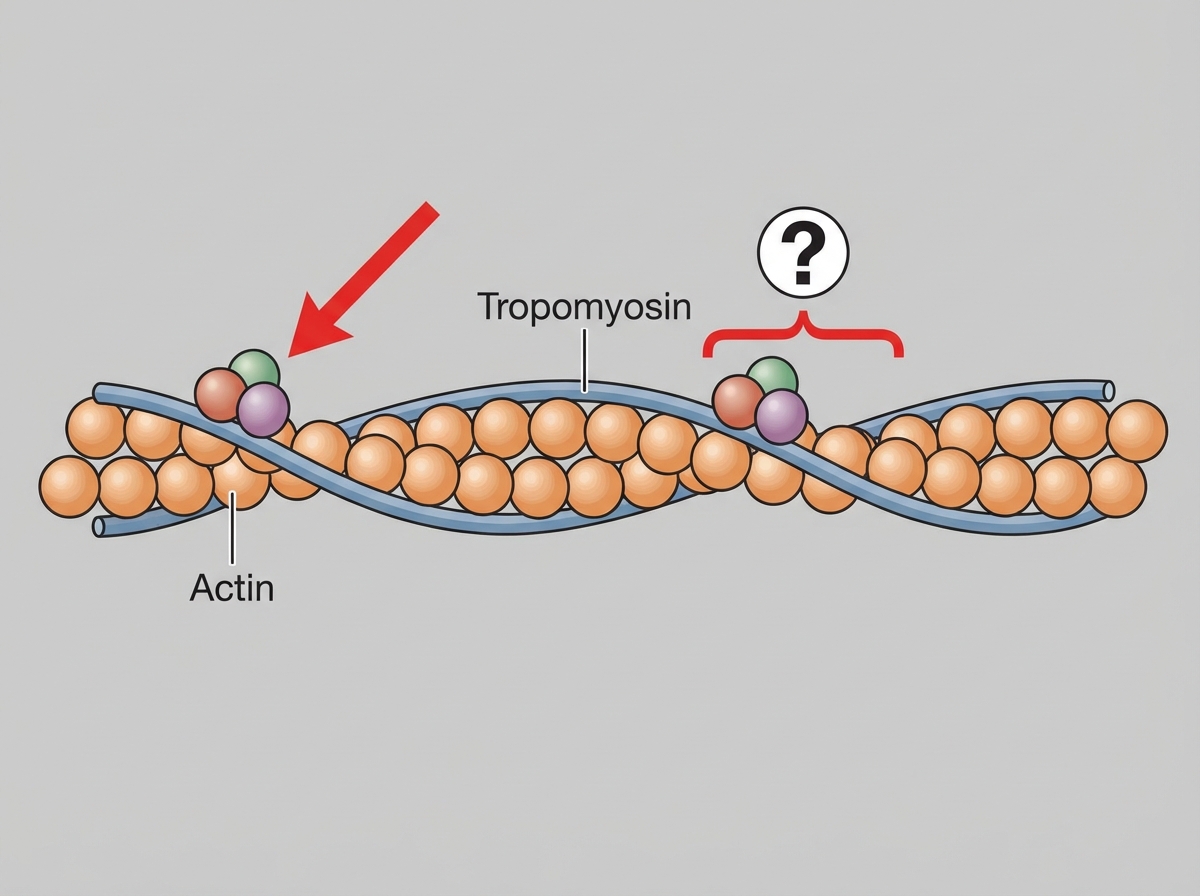
Which protein is shown in the thin filament as illustrated?
Unmyelinated nerve fibers differ from myelinated nerve fibers in that they:
Which statement about rheobase is true?
Absolute refractory period is due to which of the following?
What is true about the Golgi tendon organ?
Practice by Chapter
Resting Membrane Potential
Practice Questions
Action Potential Generation and Propagation
Practice Questions
Neuromuscular Junction
Practice Questions
Skeletal Muscle Contraction
Practice Questions
Smooth Muscle Physiology
Practice Questions
Cardiac Muscle Properties
Practice Questions
Muscle Metabolism and Fatigue
Practice Questions
Motor Unit Function
Practice Questions
Neurotransmitters and Receptors
Practice Questions
Electrophysiological Measurements
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app