
Nerve and Muscle Physiology — MCQs

On this page
A Strength-Duration curve is plotted for a skeletal muscle. Identify the parameters labeled in the correct order to successfully determine the tissue excitability.
Why is no new impulse generated during the depolarization phase of an action potential?
Based on the provided image of a nerve action potential, at which marked point is the combined transport of Na+ and K+ ions at its minimum?
Intercalated disc is composed of: 1. Cadherins 2. Desmosomes 3. Gap junctions 4. Tight junctions
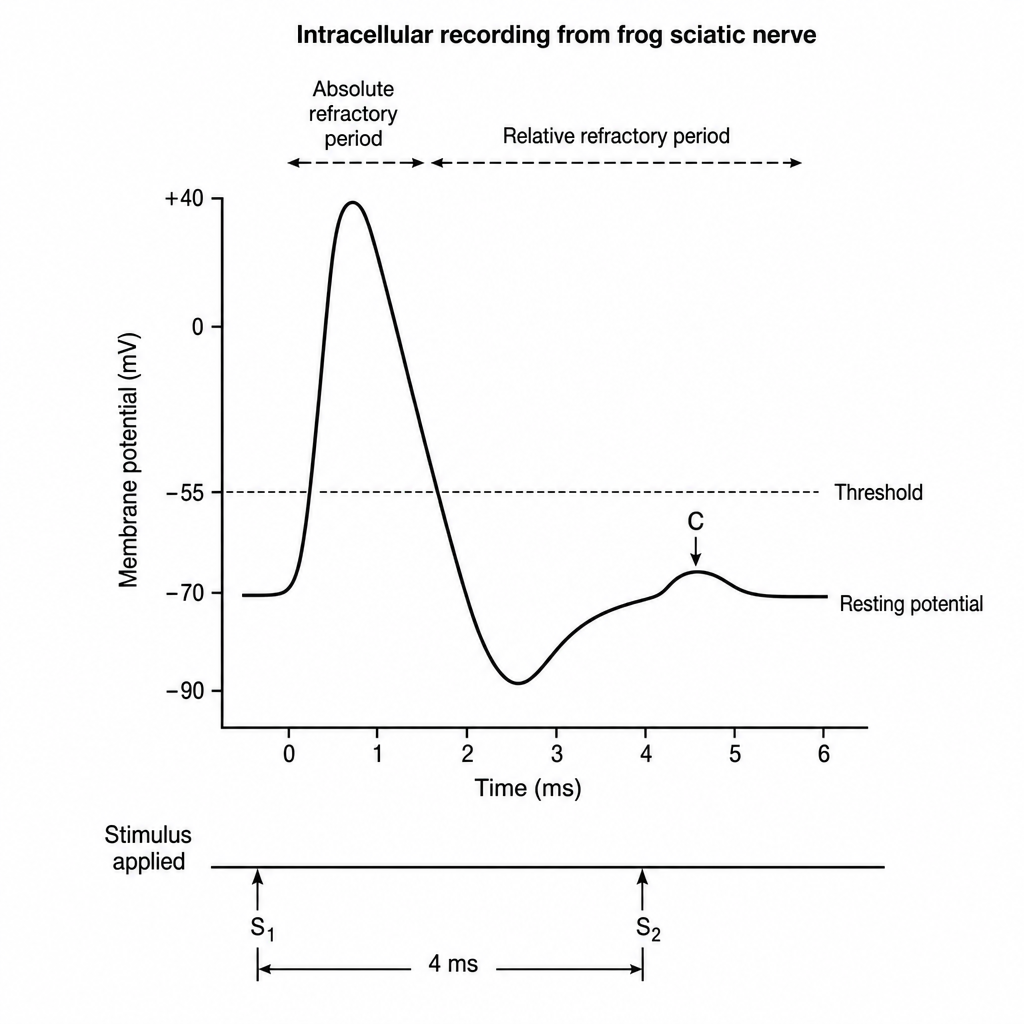
During a neurophysiology practical, a student applies two successive electrical stimuli to an isolated frog sciatic nerve preparation. The first stimulus is suprathreshold. The second stimulus, applied 4 milliseconds after the first (corresponding to the relative refractory period in this preparation), is stronger than the original suprathreshold stimulus, and is delivered at point C shown on the waveform. The recorded intracellular waveform is displayed on the oscilloscope (Image 1). Which of the following best explains the membrane state at the time the second stimulus was delivered?
Type I muscle fibers are rich in myosin heavy chain. What is their characteristic property?
The number of muscle fibers innervated by a single motor axon is smallest in which of the following?
What is the relationship between nerve thickness and conduction velocity of myelinated nerves?
In tetany, what causes the increased membrane excitability?
TTX-resistant sodium channels are caused by the involvement of which of the following?
Practice by Chapter
Resting Membrane Potential
Practice Questions
Action Potential Generation and Propagation
Practice Questions
Neuromuscular Junction
Practice Questions
Skeletal Muscle Contraction
Practice Questions
Smooth Muscle Physiology
Practice Questions
Cardiac Muscle Properties
Practice Questions
Muscle Metabolism and Fatigue
Practice Questions
Motor Unit Function
Practice Questions
Neurotransmitters and Receptors
Practice Questions
Electrophysiological Measurements
Practice Questions
Want unlimited practice?
Get full access to all questions, explanations, and performance tracking.
Scan to download app